Table of Contents
Overview – Whipple’s Disease
Whipple’s disease is a rare, systemic bacterial infection caused by Tropheryma whipplei. It primarily affects the small intestine, leading to malabsorption, but may also involve joints, the heart, brain, and other organs. This disease typically presents with a constellation of nonspecific systemic and gastrointestinal symptoms, making it a diagnostic challenge. Without treatment, Whipple’s disease is uniformly fatal—early recognition and long-term antibiotic therapy are therefore critical.
Definition
Whipple’s disease is a chronic multisystem infection caused by the bacterium Tropheryma whipplei, leading to malabsorption and systemic symptoms due to infiltration of infected macrophages into various organs.
Aetiology
- Caused by: Tropheryma whipplei
- A Gram-positive, rod-shaped, actinomycete-related bacterium
- Found within macrophages (intracellular pathogen)
- Rare; mostly affects middle-aged Caucasian men
Pathophysiology
- T. whipplei infects and replicates inside tissue macrophages
- Impaired macrophage bacterial killing → systemic dissemination
- Affects:
- Small intestine (lamina propria)
- Lymph nodes
- Joints
- Brain
- Cardiopulmonary system
- Malabsorption due to villous distortion and inflammation in small bowel mucosa
Morphology
Endoscopic Findings
- Pale, shaggy-appearing duodenal mucosa
- Eroded, red, friable patches
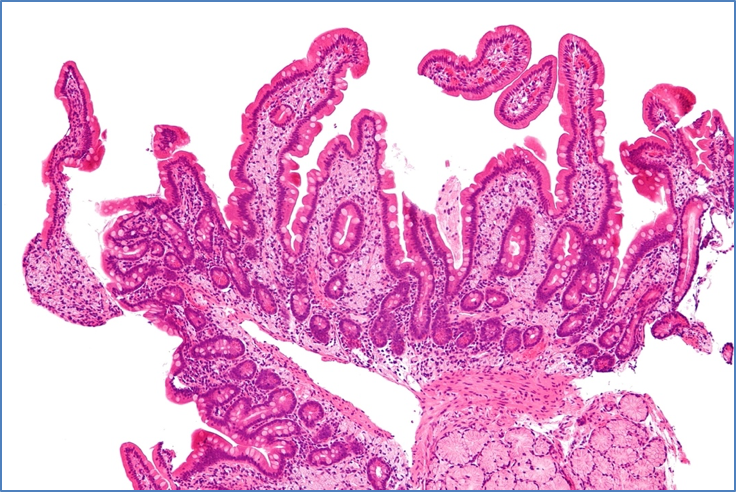
Histology
- Foamy macrophages in lamina propria containing T. whipplei
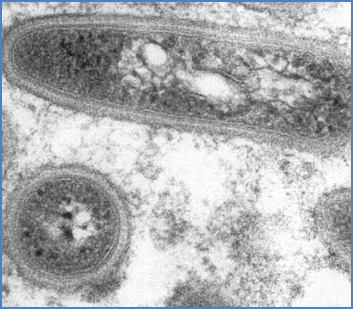
- Tri-laminar (3-layered) bacterial cell wall visible on electron microscopy
- Periodic acid–Schiff (PAS)-positive macrophages in small bowel biopsy
Clinical Features
Early Symptoms
- Arthritis and arthralgia (often migratory and the initial presentation)
Systemic Features
- Weight loss
- Diarrhoea and abdominal pain
- Fever
- Steatorrhoea (due to fat malabsorption)
- Generalised lymphadenopathy
- Neurological symptoms (late stage): dementia, ataxia, oculomotor palsies
- Cardiac: endocarditis or pericarditis
- Pulmonary: pleural effusions, cough
Investigations
- Blood tests:
- Anaemia, raised ESR/CRP
- Hypoalbuminaemia, features of malabsorption
- Endoscopy:
- Shaggy mucosa with friable erythematous patches in the duodenum
- Biopsy of duodenal mucosa:
- Foamy macrophages containing PAS-positive T. whipplei
- Electron microscopy: Tri-laminar cell walls
- Molecular tests:
- PCR for T. whipplei DNA
- Immunohistochemistry using specific antibodies
Management
- Long-term antibiotic therapy essential to prevent relapse or death
- Must include antibiotics that cross the blood–brain barrier (BBB)
- E.g. Co-trimoxazole (trimethoprim-sulfamethoxazole) for at least 12 months
- Alternatives include ceftriaxone followed by oral regimens
- Monitor neurological status for relapse
Prognosis
- Excellent with early and adequate treatment
- Fatal if untreated due to multisystem involvement
Summary – Whipple’s Disease
Whipple’s disease is a rare systemic infection caused by Tropheryma whipplei, characterised by foamy macrophages in the intestinal lamina propria and multisystem involvement. It presents with arthralgia, diarrhoea, weight loss, and neurological or cardiac symptoms in later stages. Diagnosis is based on duodenal biopsy and PCR, and treatment requires long-course antibiotics that cross the blood–brain barrier. For more infectious conditions, see our Microbiology & Public Health Overview page.