Table of Contents
Overview – Hand Examination
The hand examination is a crucial OSCE skill for evaluating joint, nerve, vascular, and soft tissue abnormalities of the hand and wrist. It is commonly tested in rheumatology, neurology, and orthopaedic stations. A systematic approach—beginning with inspection and palpation, followed by movement testing, vascular/neurological assessment, and special manoeuvres—enables the detection of conditions such as rheumatoid arthritis, carpal tunnel syndrome, Dupuytren’s contracture, psoriatic arthritis, and nerve palsies. This guide provides a concise and high-yield framework for the hand examination.
Definition
The hand examination assesses for musculoskeletal, neurological, vascular, or dermatological pathologies affecting the hands and wrists. It includes both functional and structural evaluation through observation, palpation, movement testing, and clinical tests.
Preparation
- Wash hands and introduce yourself.
- Confirm the patient’s name and age.
- Explain the exam and obtain consent.
- Position the patient seated comfortably with hands supported on a pillow, arms exposed up to the elbows.
Inspection
Compare both hands for symmetry and abnormalities:
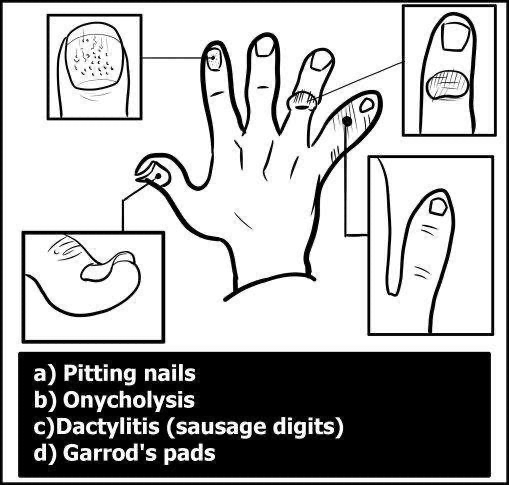
Nails
- Pitting, onycholysis → Psoriatic arthritis
- Splinter haemorrhages → Vasculitis, infective endocarditis, RA
Fingers, Hands, Wrists (Dorsum)
Swelling
- Heberden’s nodes at DIP, Bouchard’s nodes at PIP → Osteoarthritis
- MCP swelling → Rheumatoid arthritis (RA)
- Dactylitis (“sausage digit”) → Psoriatic arthritis
- Garrod’s pads → Dupuytren’s contracture
Deformities
- RA:
- Ulnar deviation of fingers
- Radial deviation of wrist
- Swan neck and boutonnière deformities
- Z-shaped thumb
- Vaughan-Jackson syndrome (extensor tendon rupture)
- Others:
- Mallet finger
- Partial or complete claw hand (ulnar nerve, Klumpke’s palsy)
- Dinner fork deformity → Colles fracture

Muscle Atrophy
- Interosseous wasting → RA, T1 root lesion, ulnar nerve palsy
- Thenar wasting → Median nerve (carpal tunnel syndrome)
- Hypothenar wasting → Ulnar nerve
Skin and Scars
- Erythema → Cellulitis, inflammation
- Palmar erythema → RA, liver disease
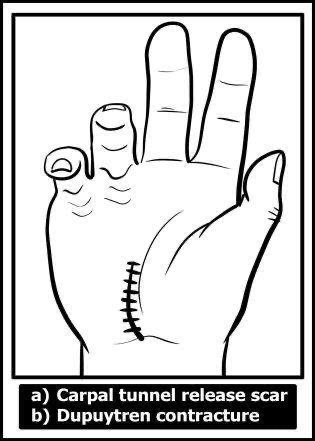
- Scars → Carpal tunnel release, Dupuytren’s surgery (Z-shaped)
- Dupuytren’s contracture → Fixed flexion of 4th/5th fingers
Other
- Psoriatic plaques (elbows, scalp)
- Gouty tophi (ears, fingers)
- Raynaud’s phenomenon → Triphasic colour change
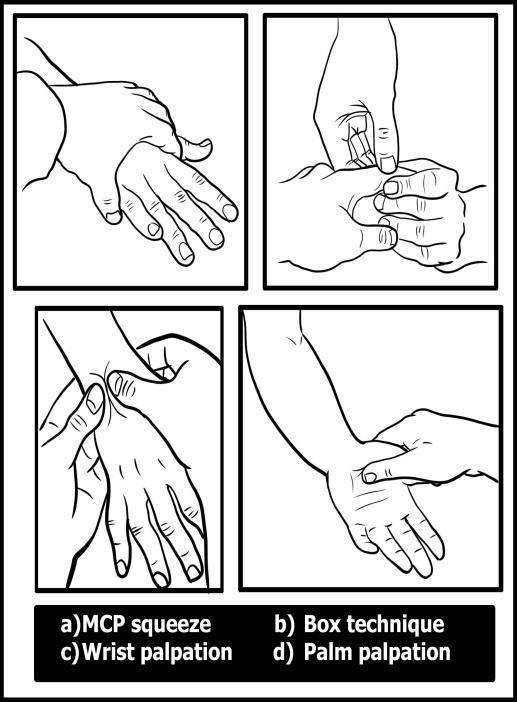
Palpation
- Temperature – Use dorsum of hands
- Tenderness & swelling – Watch facial expression
Sequence
- Elbows – Rheumatoid nodules
- Wrists – Distal radius/ulna tenderness (e.g. Colles fracture), De Quervain’s tenosynovitis (radial styloid)
- MCP joints – Squeeze test for synovitis
- PIP/DIP – Use “box” technique (all sides simultaneously)
- Palmar fascia – Thickening (Dupuytren’s)
- Flexor tendons – Nodules in trigger finger
- Snuffbox tenderness – Suspect scaphoid fracture
Movement Testing
Wrist
- Flexion (prayer sign)
- Extension (reverse prayer sign)
- Radial deviation (adduction)
- Ulnar deviation (abduction)
Fingers
- Flexion, extension, abduction, adduction
- Note trigger fingers (inability to fully extend)
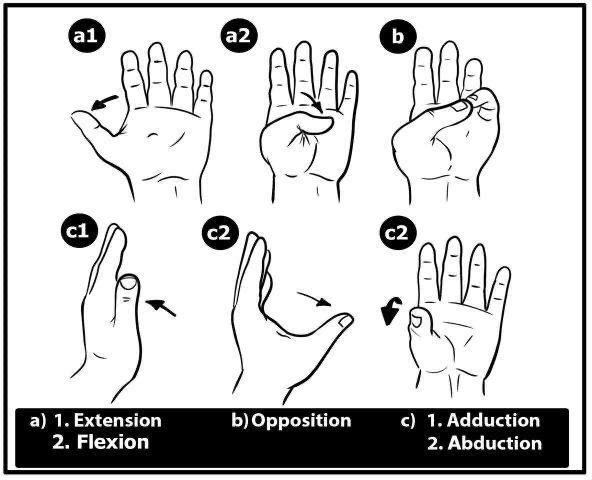
Thumb
- Flexion, extension
- Abduction, adduction
- Opposition

Vascular & Neurological Assessment
Vascular
- Capillary refill
- Radial & ulnar pulses
- Allen’s test – Assess arterial patency before cannulation
Neurological – “Paper, Scissors, Stone”
Motor (resisted testing)
- Thumb abduction → Median nerve
- Finger extension → Radial nerve
- Finger abduction → Ulnar nerve
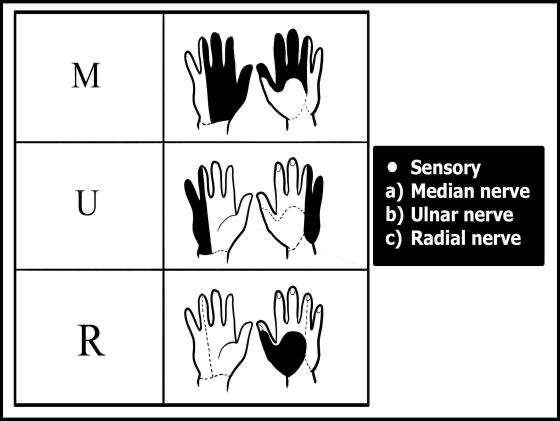
Sensory
- Median – Tip of index finger
- Ulnar – Tip of little finger
- Radial – Dorsal web space between thumb and index
Function
- Undo a button
- Pick up a coin
- Power grip (squeeze fingers)
Special Tests
Carpal Tunnel Syndrome (Median Nerve)
- Tinel’s sign – Tap over flexor retinaculum
- Phalen’s test – Reverse prayer for 60 seconds
- Durkan’s test – Direct pressure over carpal tunnel
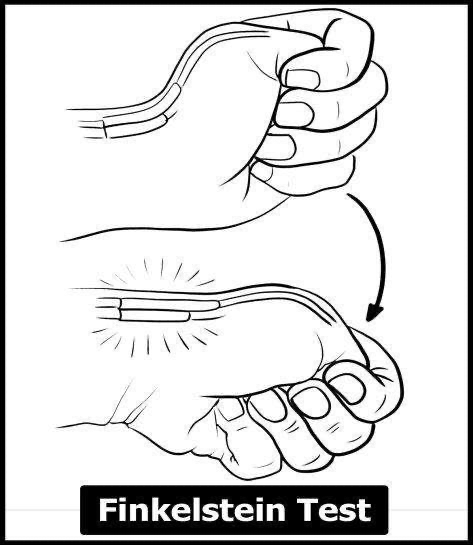
De Quervain’s Tenosynovitis
- Finkelstein test – Fist with thumb inside, ulnar deviation → pain at radial styloid
Ulnar Nerve
- Froment’s sign – Pull paper from thumb-index pinch → thumb flexion = positive
- Wartenberg’s sign – Involuntary abduction of little finger
- Tabletop test – Inability to lay palm flat on table
Common Conditions
Carpal Tunnel Syndrome
- Presentation: Nocturnal paresthesia, thenar wasting
- Causes: Pregnancy, RA, hypothyroidism, amyloidosis, idiopathic
- Management: Splints, NSAIDs, steroid injection, carpal tunnel release
Dupuytren’s Contracture
- Presentation: Painless palmar nodules, fixed flexion of fingers (esp. 4th/5th)
- Causes: Genetic, diabetes, alcohol, epilepsy
- Management: Collagenase, fasciectomy, needle fasciotomy
Rheumatoid Arthritis
- Features: Symmetrical polyarthritis (MCP, PIP, wrist), morning stiffness >1 hour
- Deformities: Swan neck, boutonnière, Z-thumb, ulnar deviation
- Extra-articular: Sjögren’s, lung fibrosis, pericarditis, vasculitis, anemia
- Investigations: Anti-CCP (specific), RF, ESR/CRP, X-ray (erosions, osteopenia)
- Management:
- NSAIDs, steroids
- DMARDs: Methotrexate (avoid alcohol), sulfasalazine, hydroxychloroquine
- Biologics: TNF inhibitors, Rituximab (screen for TB)
- Surgery: Synovectomy, joint replacement
- Disease activity: DAS28, ACR-EULAR criteria
Summary – Hand Examination
The hand examination is a high-yield OSCE station encompassing joint, nerve, vascular, and soft tissue assessment. From detecting signs of rheumatoid arthritis to evaluating carpal tunnel syndrome and Dupuytren’s contracture, it provides critical insights into systemic and localized pathologies. For a broader context, see our Clinical Skills Overview page.