Table of Contents
Overview – Congenital Heart Defects
Congenital heart defects are structural abnormalities in the heart present from birth. These include acyanotic shunts like VSD and ASD, cyanotic defects like Tetralogy of Fallot, and obstructive conditions such as coarctation of the aorta. This guide covers embryological development, postnatal circulatory changes, clinical presentations, investigations, and management options. Essential for paediatrics, cardiology, and exam preparation.
Foetal Circulation Review
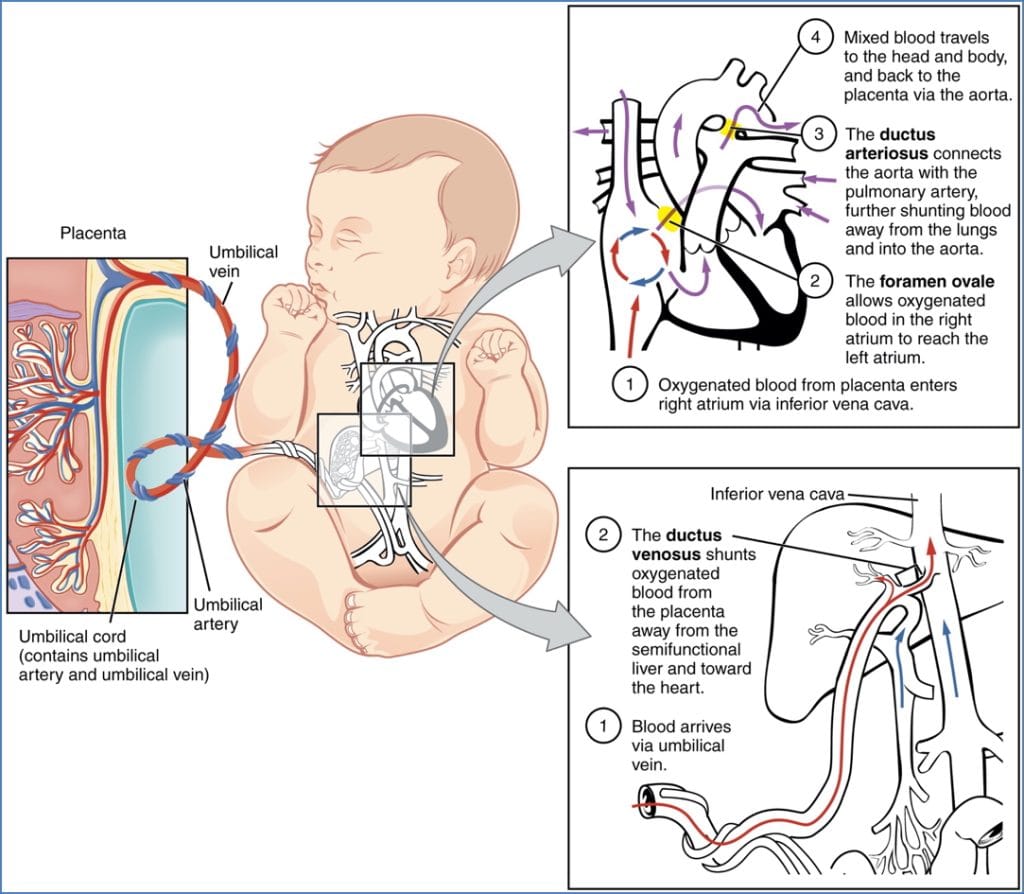
Key Shunts
- Ductus Venosus
- Shunts oxygenated blood from the placenta → inferior vena cava → right atrium
- Bypasses the liver
- Foramen Ovale
- Shunts blood from the right atrium → left atrium
- Bypasses the lungs
- Ductus Arteriosus
- Shunts blood from the pulmonary artery → aorta
- Also bypasses the lungs
All three shunts typically close postnatally due to changes in vascular pressure.
Note: The foramen ovale may take up to 6 months to fully close.
Postnatal Adaptation
- Pulmonary vascular resistance falls due to:
- Lung inflation → increases vessel radial traction
- Oxygen-mediated pulmonary vasodilation
Congenital Heart Defects
- Innocent Murmurs: Occur in ~50–80% of children; usually benign
- Red Flag: Any murmur with accompanying cyanosis or signs of hypoperfusion
Classification of Defects
- Left-to-Right (Non-Cyanotic) Shunts:
- Atrial septal defect (ASD)
- Ventricular septal defect (VSD) – most common
- Patent ductus arteriosus (PDA)
- Right-to-Left (Cyanotic) Shunts:
- Tetralogy of Fallot
- Transposition of the Great Arteries
- Obstructive Defects:
- Coarctation of the aorta
- Valvular stenoses (aortic, pulmonary)
Genetic Associations
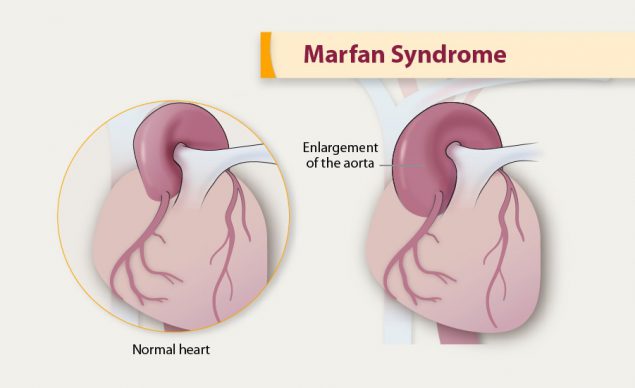
Marfan Syndrome
- Autosomal dominant connective tissue disorder
- Associated cardiac anomalies:
- Aortic aneurysms
- Mitral or tricuspid valve prolapse
- Atrial septal defects
Down Syndrome (Trisomy 21)
- ~40% of affected individuals have congenital heart defects
- Common cardiac anomalies:
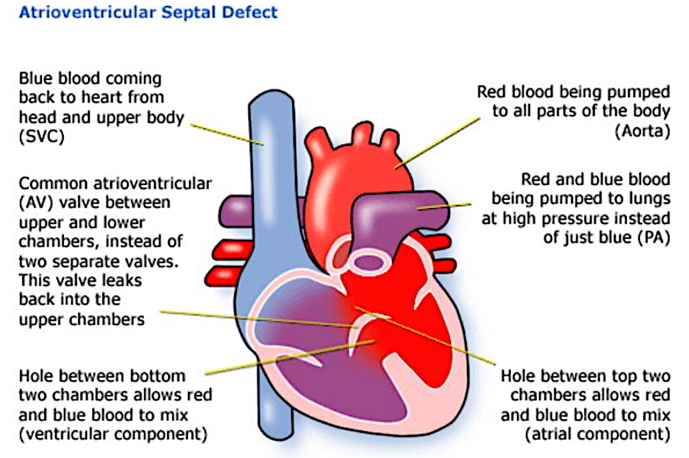
- Atrioventricular septal defects (AVSD)
- Valvular malformations
- Combined ASD + VSD
Left-to-Right Shunts
Patent Ductus Arteriosus (PDA)
- Definition: Failure of ductus arteriosus to close after birth.
- Shunt: Blood flows from aorta → pulmonary artery.
- Mechanism: Caused by persistently high prostaglandins or insufficient oxygen-mediated closure.
- Clinical Features:
- Continuous, harsh “machinery-like” murmur
- Complications:
- Pulmonary hypertension
- Irreversible obstructive pulmonary vascular disease
- Shunt reversal → cyanosis
- Investigations:
- CXR: Cardiomegaly, pulmonary congestion
- ECG: Left and right ventricular hypertrophy
- Echocardiography: Diagnostic
- Management:
- Medical: Indomethacin (prostaglandin inhibitor) to promote closure
- Note: In cyanotic heart defects, prostaglandin is used to keep PDA open
- Surgical: Ligation of the ductus arteriosus
- Timing: Closure should occur as early as possible to prevent complications
- Medical: Indomethacin (prostaglandin inhibitor) to promote closure

Atrial Septal Defect (ASD)
- Definition: A persistent opening in the interatrial septum (distinct from a patent foramen ovale)
- Shunt: Left atrium → right atrium
- Mechanism: Pressure gradient between atria increases right-sided volume load
- Clinical Features:
- Often asymptomatic in childhood
- Murmurs:
- Diastolic murmur (atrial contraction)
- Systolic pulmonary flow murmur (hyperdynamic)
- Wide, fixed splitting of second heart sound (delayed pulmonary valve closure)
- RV heave (parasternal) due to hypertrophy
- Complications:
- Congestive cardiac failure (dyspnoea, oedema, ascites)
- Paradoxical embolism (e.g., stroke from deep vein thrombosis)
- Investigations:
- ECG: Right ventricular hypertrophy, right axis deviation
- CXR: Pulmonary congestion
- Echocardiography: Definitive diagnosis
- Management:
- Percutaneous or surgical closure

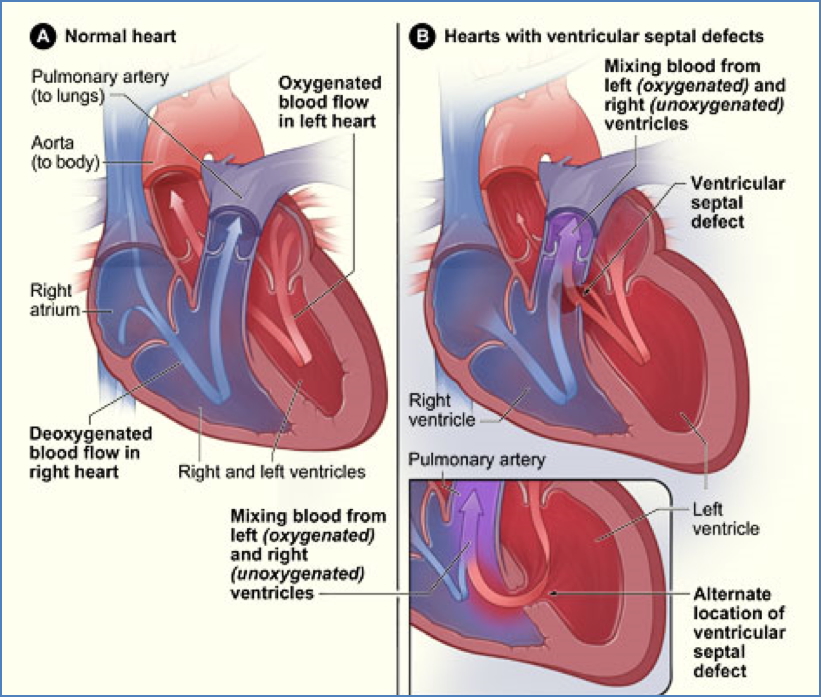
Ventricular Septal Defect (VSD)
- Definition: A hole in the interventricular septum; most common congenital heart defect
- Shunt: Left ventricle → right ventricle
- Mechanism: High left-sided pressure causes blood to enter the lower-pressure right ventricle
- Clinical Features:
- Small VSD: Often asymptomatic, may close spontaneously
- Large VSD:
- Failure to thrive
- Congestive cardiac failure (dyspnoea, cough, oedema)
- Murmurs:
- Pansystolic murmur ± left sternal thrill
- Pulmonary flow murmur
- Complications:
- Pulmonary hypertension → RV hypertrophy
- Shunt reversal → right-to-left flow → cyanosis (Eisenmenger’s syndrome)
- Investigations:
- CXR: Cardiomegaly, pulmonary congestion
- ECG: Left and right ventricular hypertrophy
- Echocardiography: Definitive diagnosis
- Management:
- Early surgical closure is essential for a normal lifespan
Right-to-Left Shunts (Cyanotic – SpO2 <75%)
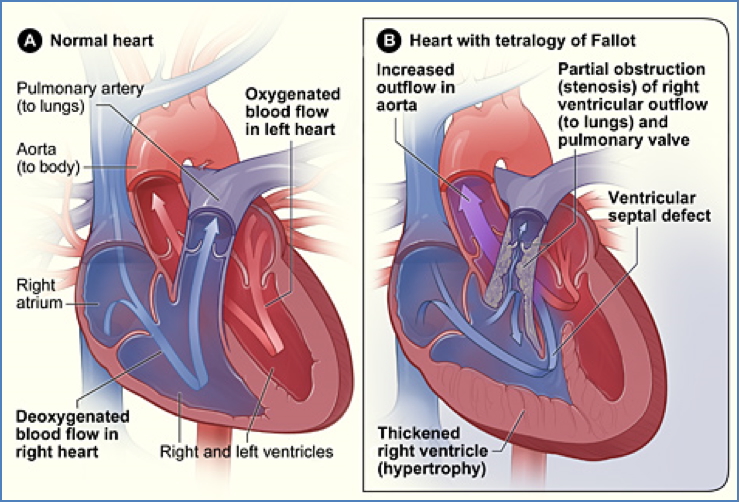
Tetralogy of Fallot
- Definition: A cyanotic congenital heart defect with four cardinal features:
- Ventricular septal defect (VSD)
- Overriding aorta – straddles the VSD, receiving blood from both ventricles
- Pulmonary stenosis – subvalvular or valvular obstruction to right ventricular outflow
- Right ventricular hypertrophy – secondary to increased workload
- (Fifth feature sometimes: Patent ductus arteriosus)
- Pathophysiology:
- Severe pulmonary stenosis → RV pressure exceeds LV → R-L shunting of deoxygenated blood → hypoxaemia
- Clinical Features:
- Mild stenosis: Non-cyanotic, resembles isolated VSD
- Severe stenosis:
- Cyanosis (SpO₂ <75%)
- Finger clubbing
- Polycythaemia (↑RBC production due to chronic hypoxia)
- Paroxysmal tachypnoea, irritability, “blue baby” presentation
- Classical finding: Relief of symptoms by squatting – increases systemic vascular resistance → improves pulmonary blood flow
- Complications:
- Paradoxical embolism (e.g. stroke from venous clot)
- Seizures from hypoxia
- Investigations:
- ECG: Right ventricular hypertrophy
- CXR: Boot-shaped heart (right ventricular prominence)
- Echocardiography: Definitive
- Management:
- Medical: Oxygen, beta-blockers
- Surgical: Complete repair (usually within the first year of life)
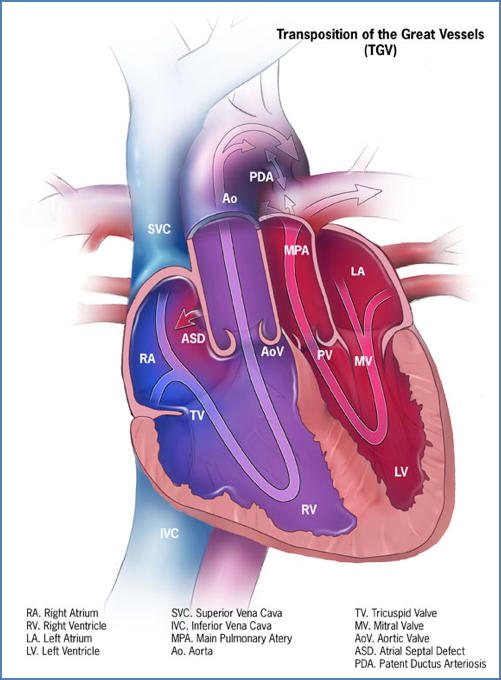
Transposition of the Great Vessels (TGV)
- Definition: A condition in which the aorta arises from the right ventricle and the pulmonary artery arises from the left ventricle
- Atrioventricular and venous connections are normal
- Pathophysiology:
- The pulmonary and systemic circulations operate in parallel, not in series → no oxygenated blood reaches systemic tissues unless a mixing lesion (e.g. PDA, VSD) is present
- Clinical Features:
- Most common cause of cyanosis in neonates
- Cyanosis within hours of birth
- Clubbing, polycythaemia due to chronic hypoxia
- Complications:
- Right ventricular hypertrophy (pressure overload)
- Left ventricular atrophy (underuse)
- Investigations:
- ECG: Right axis deviation, RVH
- CXR: “Egg on a string” heart (narrow mediastinum)
- Echocardiography: Diagnostic
- Management:
- Prostaglandin E1 infusion to maintain PDA and ensure mixing
- Balloon atrial septostomy (temporary)
- Arterial switch operation (definitive)
- Prognosis:
- Without intervention:
- 30% die within 1 week
- 90% die within 1 year
- Surgical correction dramatically improves outcomes
- Without intervention:
‘Obstructive’ Congenital Heart Defects
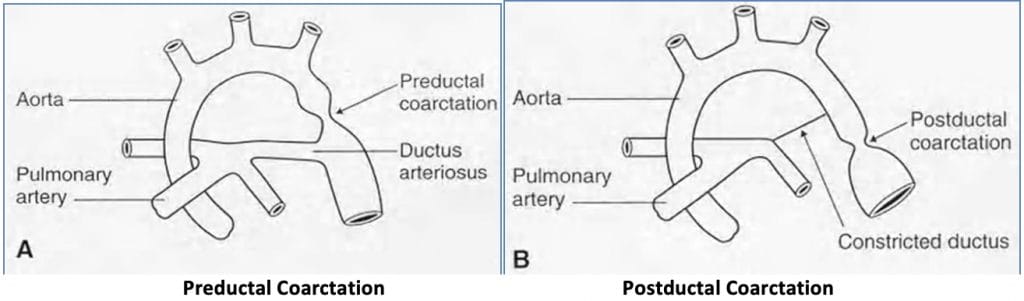
Coarctation of the Aorta
- Definition: Narrowing (coarctation) of the aortic arch, typically near the ductus arteriosus
- Epidemiology:
- Male:female ratio = 2:1
- 50% have coexisting bicuspid aortic valve
- Pathophysiology:
- Pre-ductal Coarctation:
- Narrowing proximal to the ductus arteriosus
- Results in right-to-left shunt (pulmonary artery to aorta)
- Cyanosis in lower half of the body
- Post-ductal Coarctation:
- Narrowing distal to the ductus arteriosus
- Causes left-to-right shunt (aorta to pulmonary artery)
- Pulmonary hypertension and congestive cardiac failure
- Overall Effects:
- ↑Afterload → ↑Left ventricular end-systolic volume → ↓Cardiac output → Hypotension
- Backup in lungs → Pulmonary congestion
- Left ventricular hypertrophy and potential failure
- Reduced perfusion to abdominal organs and lower limbs
- Pre-ductal Coarctation:
- Clinical Features:
- Symptoms:
- Leg claudication, cold extremities
- Delayed presentation (usually >10 years old) due to progressive mismatch between growth and aortic flow
- Signs:
- Upper limb BP > lower limb BP
- Radiofemoral delay
- Systolic murmur
- Cold legs, prolonged capillary refill
- Left ventricular hypertrophy
- Symptoms:
- Investigations:
- ABI (Ankle-Brachial Index): asymmetrical
- ECG: Left ventricular hypertrophy
- Management:
- Surgical correction (e.g. balloon angioplasty and stenting)

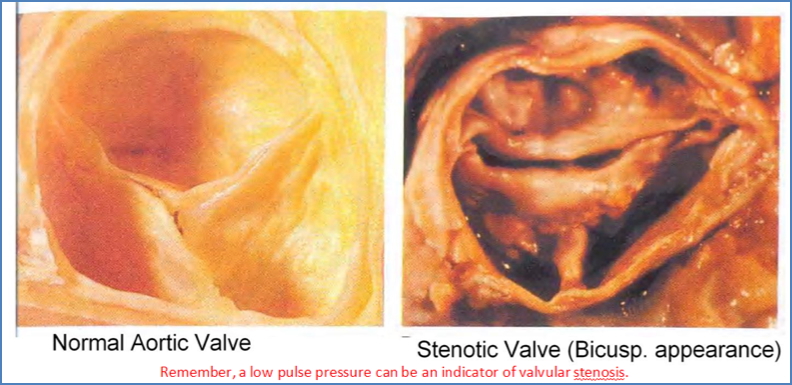
Aortic Stenosis
- Definition: Congenital narrowing of the aortic valve
- Anatomy: Usually bi-leaflet (instead of normal tri-leaflet structure)
- Epidemiology: More common in males
- Pathophysiology:
- Increased left ventricular afterload
- Decreased cardiac output
- Risk of left-sided heart failure and pulmonary hypertension
- Clinical Manifestations:
- Dyspnoea, chest pain, syncope, murmur
Pulmonic Stenosis
- Definition: Obstruction of the pulmonary valve or pulmonary artery
- Anatomy:
- 90% valvular
- 10% subvalvular or supravalvular
- Pathophysiology:
- Increased right ventricular afterload
- Decreased pulmonary blood flow
- Right ventricular failure → peripheral oedema
- Clinical Manifestations:
- May include murmur, fatigue, hepatomegaly

Summary – Congenital Heart Defects
Congenital heart defects span a wide clinical spectrum from asymptomatic murmurs to life-threatening cyanosis. Understanding their embryologic origin, pathophysiology, and progression helps distinguish between acyanotic and cyanotic conditions, guides timely diagnosis, and informs surgical or medical management.
Interested in more topics from the cardiovascular system? Explore our Cardiovascular Overview for anatomy, physiology, and pathology summaries.