Table of Contents
Overview – Acute Myeloid Leukaemia
Acute Myeloid Leukaemia (AML) is an aggressive malignancy of myeloid progenitor cells (myeloblasts), leading to uncontrolled proliferation, bone marrow failure, and systemic symptoms. It is most common in adults, especially the elderly, and carries a poorer prognosis than ALL. Rapid diagnosis and initiation of chemotherapy are essential for survival.
Definition
- Malignant clonal disorder of myeloblasts
- Leads to bone marrow failure and widespread infiltration of tissues
- Characterised by >20% myeloblasts in bone marrow or peripheral blood
Aetiology
- De novo AML: No preceding haematological disorder
- Secondary AML: Progression from:
- Myelodysplastic syndromes
- Myeloproliferative neoplasms
- Previous chemotherapy (alkylating agents, topoisomerase inhibitors)
- Risk factors:
- Radiation exposure
- Benzene, smoking
- Genetic syndromes (e.g. Down syndrome)
Pathophysiology
- Genetic mutations in myeloid stem cells →
- Arrested maturation
- Accumulation of immature myeloblasts
- Suppression of normal haematopoiesis → Anaemia, thrombocytopenia, neutropenia
- Infiltration into liver, spleen, lymph nodes, gums, and CNS
Clinical Features
- Demographics: Most common in older adults
- Symptoms:
- Bone pain (especially sternum)
- Constitutional symptoms (fatigue, weight loss)
- Anaemia → pallor, dyspnoea
- Thrombocytopenia → easy bruising, bleeding
- Neutropenia → frequent infections
- Gum hypertrophy (especially monocytic AML subtypes)
- Signs:
- Hepatosplenomegaly
- Lymphadenopathy
- Fever
- Petechiae, mucosal bleeding
Investigations
- FBC:
- Anaemia (↓ Hb), Thrombocytopenia (↓ Plts), ↑ or ↓ WCC
- Circulating blast cells
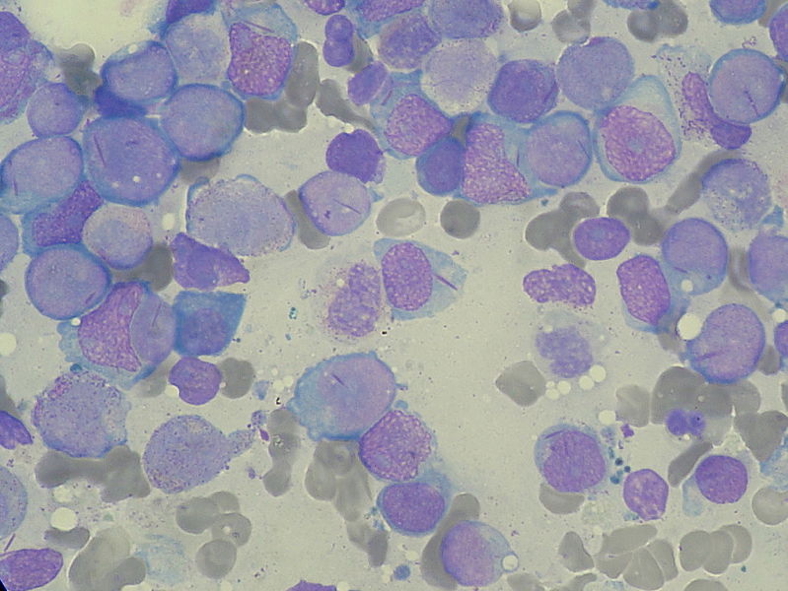
- Blood film:
- Myeloblasts, possibly with Auer rods (pathognomonic)
- Bone marrow biopsy:
- 20% blasts required for diagnosis
- Confirm presence of Auer rods
- Cytogenetics:
- Determines prognosis and treatment strategy
- Favourable: t(8;21), inv(16), t(15;17)
- Cytochemistry:
- Myeloperoxidase and Sudan Black → Positive in AML (Negative in ALL)
- CXR/CT:
- Evaluate for mediastinal mass, lymphadenopathy, or infection
Management
- Supportive care:
- Blood and platelet transfusions
- Antibiotics, antivirals, antifungals
- Tumour lysis syndrome prophylaxis (hydration, allopurinol)
- Chemotherapy:
- Induction: “7+3” regimen (cytarabine + anthracycline)
- Consolidation: high-dose cytarabine or stem cell transplant
- Allogeneic stem cell transplant:
- Curative potential for high-risk or relapsed patients
Prognosis
- Poorer than ALL
- Mortality increases with age
- Prognostic factors include:
- Cytogenetics
- Age
- Response to induction therapy
Summary – Acute Myeloid Leukaemia
Acute Myeloid Leukaemia (AML) is a life-threatening malignancy of myeloblasts, often presenting with bone marrow failure and systemic signs. Diagnosis relies on blood film, bone marrow biopsy, and cytogenetics. Prompt treatment with chemotherapy and possible stem cell transplant is crucial. For more haematological topics, refer to our Blood & Haematology Overview page.