Table of Contents
Overview – SIADH
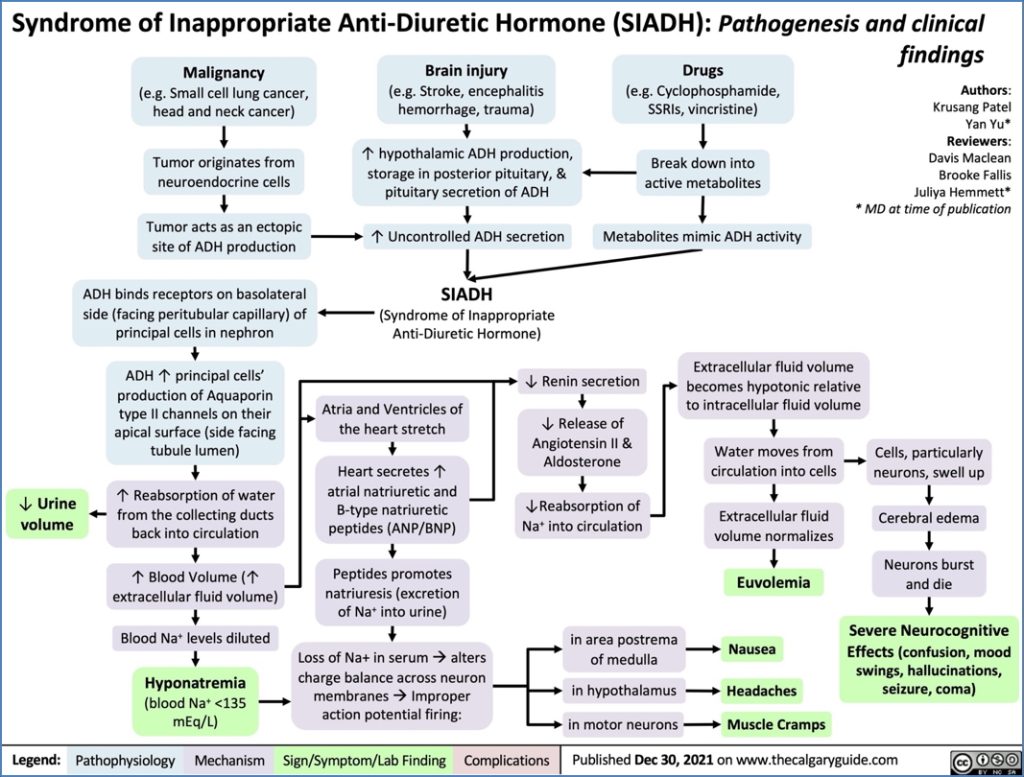
Syndrome of Inappropriate Antidiuretic Hormone secretion (SIADH) is a condition of excessive ADH activity, causing water retention and dilutional hyponatraemia despite normal or low plasma osmolality. It arises when ADH secretion is not suppressed appropriately, either due to osmoreceptor dysfunction, ectopic hormone production, or other secondary triggers. SIADH is clinically significant as it can lead to severe electrolyte disturbances and neurological complications if untreated.
Definition
SIADH is defined by the inappropriate, persistent release of antidiuretic hormone (ADH), leading to water retention, dilutional hyponatraemia, and concentrated urine despite low plasma osmolality.
Aetiology
Primary Mechanism
- Insensitivity of hypothalamic osmoreceptors to ↓ plasma osmolality → continued ADH secretion despite hypo-osmolality
Secondary Causes
- Malignancy (most notably small cell lung carcinoma – ectopic ADH production)
- CNS pathology (e.g., head trauma, stroke, brain tumour, infection)
- Pulmonary disease (e.g., pneumonia, tuberculosis)
- Drugs:
- Endocrine disorders:
- Hypothyroidism
- Adrenal insufficiency
Pathophysiology
- Excess ADH promotes water reabsorption in the collecting ducts
- This dilutes serum sodium concentration, causing dilutional hyponatraemia
- Despite fluid retention, no peripheral oedema develops due to sodium loss through natriuresis
- Plasma osmolality is low; urine osmolality remains inappropriately high
Clinical Features
5 Cardinal Features
- Fluid Overload (but no peripheral oedema or hypertension)
- Hyponatraemia (Dilutional) →
- Headache
- Nausea & vomiting
- Lethargy
- Confusion
- Seizures (if severe)
- Coma (late-stage/severe)
- Natriuresis – increased sodium excretion in urine
- High Urine Osmolality relative to plasma
- Normal renal and adrenal function
Investigations
- Serum sodium: ↓
- Serum osmolality: ↓
- Urine sodium: ↑
- Urine osmolality: ↑ (inappropriately concentrated)
- Assess thyroid and adrenal function to rule out mimics
Management
General Approach
- Treat the underlying cause (e.g., remove offending drug or treat infection)
First-Line
- Fluid restriction – typically <1L/day
- Monitor sodium correction closely (to avoid central pontine myelinolysis)
Pharmacological
- Demeclocycline:
- Induces nephrogenic DI as a side effect
- Reduces kidney sensitivity to ADH
- Vaptans (ADH Receptor Antagonists):
- Conivaptan: inhibits multiple ADH receptors
- Tolvaptan: selectively blocks V2 receptors in kidney
Complications
- Seizures and coma from acute hyponatraemia
- Central pontine myelinolysis from overly rapid sodium correction
- Chronic SIADH can impair quality of life due to persistent hyponatraemia
Differential Diagnosis
- Hypothyroidism
- Adrenal insufficiency
- Primary polydipsia
- Diuretic use
- Renal salt-wasting conditions
Summary – SIADH
SIADH is a disorder of excessive ADH secretion leading to water retention, dilutional hyponatraemia, and inappropriately concentrated urine. It presents with non-oedematous fluid overload and neurological symptoms secondary to hyponatraemia. Management involves fluid restriction and ADH antagonists such as vaptans. Timely recognition is vital to prevent complications such as seizures or osmotic demyelination. For more, visit our Endocrine Overview page.