Table of Contents
Overview – Pre-Renal Failures
Pre-renal failures are a leading and reversible cause of acute kidney injury (AKI), resulting from inadequate renal perfusion without intrinsic kidney damage. Common causes include hypovolaemia, shock, and renal artery stenosis. Understanding the pathophysiology and clinical features of pre-renal failures is essential for timely recognition and management to prevent progression to intrinsic renal damage or multi-organ failure.
Definition
Pre-renal failure refers to acute kidney dysfunction secondary to decreased renal blood flow, without primary injury to the nephron structures.
Aetiology
- Any condition causing reduced renal perfusion:
- Hypovolaemia (e.g. haemorrhage, diarrhoea, vomiting, burns)
- Cardiogenic shock or heart failure (e.g. CCF, ascites)
- Systemic hypotension (e.g. septic shock)
- Renal artery/vein thrombosis or stenosis
- Severe vasoconstriction (e.g. NSAID overuse)
Pathophysiology
- ↓ Renal perfusion → ↓ GFR
→ Reduced filtration of waste products
→ Oliguria/anuria and azotaemia
→ Potential progression to acute tubular necrosis if prolonged - Ischaemia of renal parenchyma → cortical necrosis in severe cases
- ↓ Perfusion also stimulates RAAS → further vasoconstriction and sodium/water retention

Clinical Features
- Features of acute kidney injury:
- Oliguria or anuria
- Fatigue, malaise, nausea, headache (from uraemia)
- Thirst, dry mucosa (if hypovolaemic)
- Elevated serum creatinine and urea
Investigations
- Bloods:
- ↑ Urea and creatinine (U:Cr ratio >20:1 typically)
- Electrolyte imbalances (e.g. hyperkalaemia, metabolic acidosis)
- Urinalysis:
- Minimal proteinuria
- Bland sediment
- Imaging:
- Renal Doppler Ultrasound
- CT-KUB with contrast (if needed)
- MRA (if contrast contraindicated)
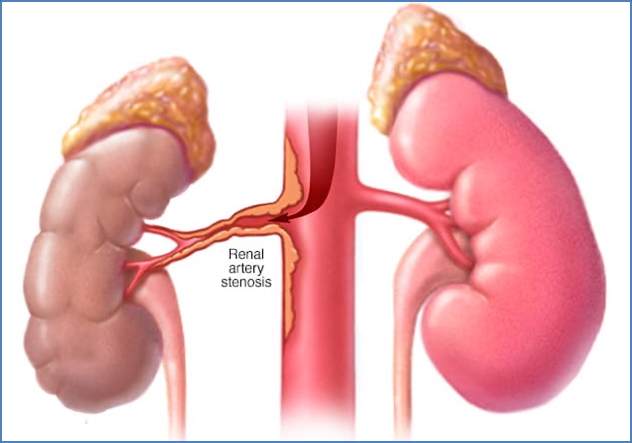
Renal Artery Stenosis
- Aetiology:
- Atherosclerosis (common in older males)
- Fibromuscular dysplasia (younger females)
- Clinical Features:
- Sudden-onset or resistant hypertension
- Headaches, blurred vision
- Renal bruit on auscultation
- Investigations:
- Doppler ultrasound
- CT angiography / MRA
- Renal arteriogram (gold standard)
- Management:
- ACE inhibitors or calcium channel blockers
- Revascularisation via angioplasty or bypass surgery
- Complications:
- Renovascular hypertension
- Progressive renal fibrosis or atrophy
- Pre-renal failure
Renal Cortical Necrosis
- Aetiology:
- Abrupt and severe hypoperfusion from:
- Disseminated intravascular coagulation (DIC)
- Vasospasm
- Septic shock
- Abrupt and severe hypoperfusion from:
- Clinical Features:
- Sudden onset flank pain
- Oliguria/anuria
- Investigations:
- CT scan without contrast
- Bloods: urea, creatinine, hyperkalaemia
- Urine: proteinuria, haematuria, casts
- Renal biopsy: patchy cortical necrosis
- Management:
- IV fluids
- Treat underlying cause
- Dialysis in severe cases
- Complications:
- Acute kidney failure
- Risk of progression to ESRD
Complications
- Acute tubular necrosis (if ischaemia persists)
- Full renal failure requiring dialysis
- Systemic complications due to uraemia, electrolyte imbalance
- Multi-organ failure (especially in septic or cardiogenic shock)
Summary – Pre-Renal Failures
Pre-renal failures result from inadequate renal blood flow and are among the most common reversible causes of acute kidney injury. Recognising the early signs such as oliguria, uraemia, and hypovolaemia is critical for timely intervention. If uncorrected, pre-renal failure can evolve into permanent nephron damage. For a broader context, see our Renal Overview page.