Table of Contents
Overview – Macrocytic Anaemia
Macrocytic anaemia is characterised by the presence of abnormally large red blood cells and elevated mean corpuscular volume (MCV). It is commonly caused by vitamin B12 or folate deficiency, which disrupt DNA synthesis during erythropoiesis, leading to the formation of large, immature erythroblasts (megaloblasts). This condition is often associated with classic clinical signs, including glossitis and peripheral neuropathy. A clear understanding of the underlying causes is critical, as macrocytic anaemia is treatable — and often reversible — with nutritional supplementation and management of the underlying disease.
Definition
- A form of anaemia with increased MCV (>100 fL)
- Often due to vitamin B12 or folate deficiency
- Also termed megaloblastic anaemia when due to defective DNA synthesis in the marrow
Aetiology
Vitamin B12 Deficiency
- Dietary deficiency (e.g. vegan diet)
- Pernicious anaemia (autoimmune destruction of gastric parietal cells → ↓ intrinsic factor)
- Ileal disease/resection (e.g. Crohn’s disease)
Folate Deficiency
- Dietary deficiency
- Malabsorption (e.g. coeliac disease, jejunal resection)
- Increased demand (e.g. pregnancy, lactation, chronic inflammation, cancer)
- Excess urinary loss (e.g. liver failure, congestive heart failure)
Other Causes
- Alcoholism and liver disease
- Cytotoxic drugs (e.g. methotrexate)
- Older age
Pathophysiology
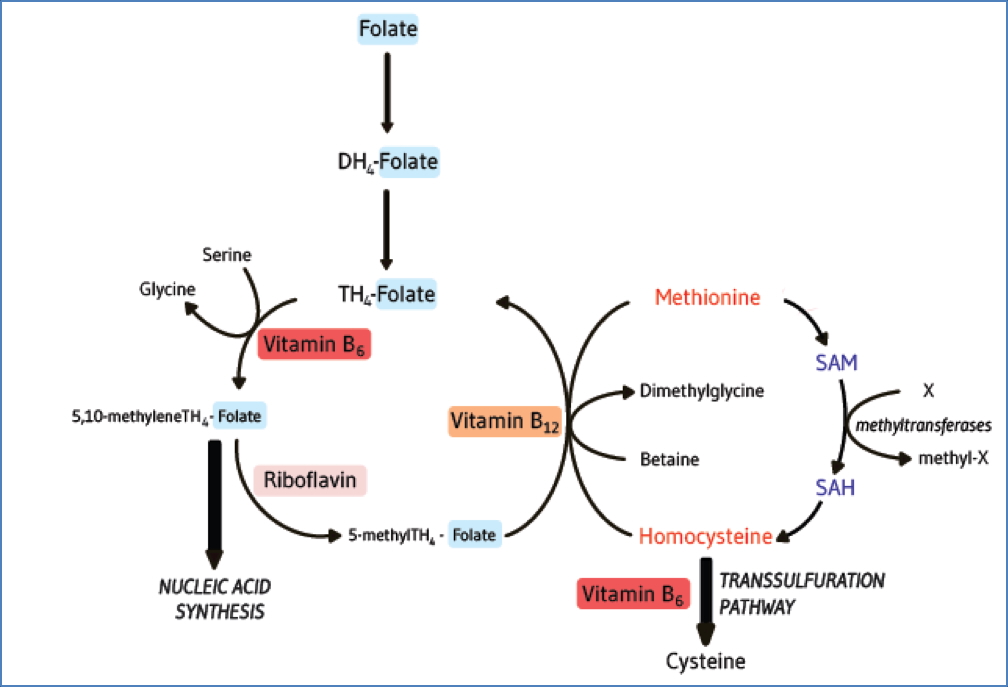
- Vitamin B12 and folate are crucial for DNA synthesis in developing RBCs
- Deficiency → impaired nuclear maturation
- Results in:
- Megaloblastic changes in the marrow
- Ineffective erythropoiesis
- Pancytopenia due to general marrow dysfunction
Morphology
Blood Film
- Normochromic macrocytes (often oval-shaped)
- Hypersegmented neutrophils (>6 lobes)
- Anisopoikilocytosis (variation in size and shape)
- Pancytopenia (↓ RBCs, WBCs, platelets)
- Polychromatophils and nucleated RBCs may be present due to marrow stress
Bone Marrow
- Megaloblasts: large erythroblasts with immature nuclei
- Bone marrow biopsy is rarely needed unless the cause is unclear

Clinical Features
General Anaemia Symptoms
- Fatigue
- Exertional dyspnoea
- Pallor
- Dizziness
Specific Features of Megaloblastic Anaemia
- Glossitis (smooth, sore tongue)
- Angular stomatitis/chelitis
- Peripheral neuropathy (B12-related):
- Paraesthesia
- ↓ Vibration and proprioception
- Weakness and ataxia
Investigations
- FBC: ↑ MCV, pancytopenia
- Blood film: macrocytes, hypersegmented neutrophils
- Serum B12 and folate levels
- Bone marrow biopsy: rarely needed; shows megaloblasts
Treatment
- Oral vitamin B12 supplementation
- Oral folate
- Corticosteroids + B12 if pernicious anaemia suspected or confirmed
- Address underlying cause (e.g. dietary changes, treat malabsorption)
Summary – Macrocytic Anaemia
Macrocytic anaemia is usually caused by vitamin B12 or folate deficiency, leading to ineffective erythropoiesis and the appearance of large, immature erythroid cells. Clinical findings may include glossitis, stomatitis, and neurological symptoms. Diagnosis involves full blood count, blood film, and serum vitamin levels. With proper treatment, including vitamin supplementation, the condition is reversible. For a broader context, see our Blood & Haematology Overview page.