Table of Contents
Overview – Knee Examination
The knee examination is a core component of musculoskeletal OSCEs and clinical assessment of joint pain, trauma, swelling, or instability. It is especially relevant for evaluating patients with ligament injuries, meniscal tears, inflammatory arthritis, or effusions. This guide provides a systematic and high-yield approach to knee examination, from inspection and palpation to special tests that help differentiate pathologies such as anterior cruciate ligament (ACL) tears, meniscal injuries, and gout.
Preparation
- Wash hands, introduce yourself, confirm patient identity and age.
- Explain procedure and gain consent.
- Patient should be in shorts, lying with bed at 45°.
- Inspect surroundings for walking aids.
Inspection
General Inspection
- Compare both knees.
- Begin with patient standing to assess:
- Gait:
- Antalgic gait → reduced stance phase (due to pain)
- Deformities:
- Varus (bow-legged) → osteoarthritis
- Valgus (knock-knees) → arthritis
- Flexion deformity → inability to fully extend the knee
- Gait:
Local Signs
- Scars:
- Small incisions (arthroscopy/meniscectomy)
- Midline incision (total knee replacement)
- Swelling & erythema → inflammation or infection
- Wasting of quadriceps:
- Measure 15 cm above superior pole of patella
- Baker’s cyst:
- Posterior swelling in popliteal fossa (RA, OA)
- Psoriatic plaques: especially over extensor surfaces
Palpation
- Temperature: Use back of hand to compare above both knees
- Tenderness sites (flex knee to 90°):
- Popliteal fossa → Baker’s cyst
- Medial/lateral joint lines → meniscus or collateral ligament injury
- Patellar borders
- Tibial tuberosity → tibial apophysitis (Osgood-Schlatter)
- Femoral condyles
Effusion Tests
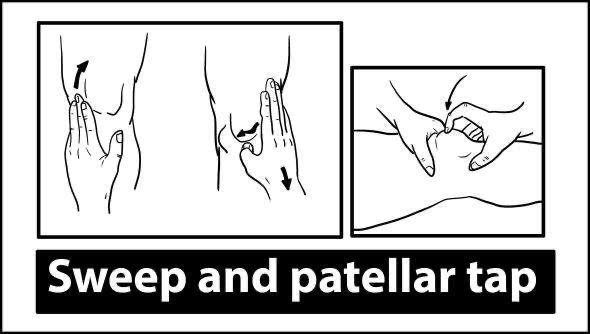
Patellar Tap (for large effusions)
- Compress suprapatellar pouch downward
- Press down patella with fingers
- Positive = floating or bouncing patella
Bulge Sign (for small effusions)
- Stroke upwards on medial aspect of knee
- Then swipe downward on lateral side
- Positive = bulge appears on medial side
Range of Motion (ROM)
Compare active vs passive movements, feel for crepitus:
- Flexion: up to 140° (biceps femoris, semitendinosus)
- Extension: full extension expected
- Hyperextension: up to 10° in some individuals
Special Tests
Ligament Stability
Anterior Drawer Test – ACL tear
- Knee flexed at 90°, sit on foot
- Pull tibia forward → excessive movement = ACL tear
Posterior Drawer Test – PCL tear
- Same position as above
- Push tibia backward
Lachman’s Test – ACL
- One hand stabilizes femur
- Other pulls tibia forward → test for anterior laxity
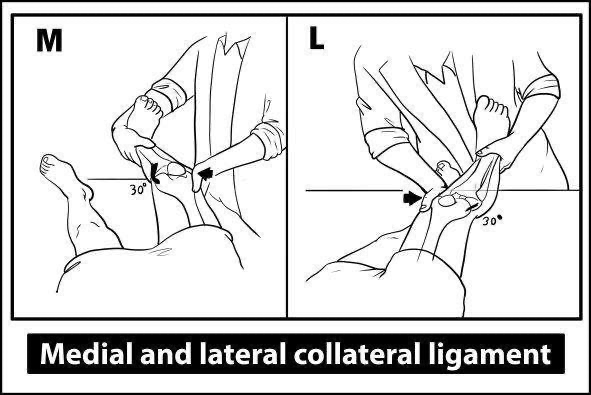
Collateral Ligament Test
- Flex knee to 30°
- Apply valgus stress (medial) and varus stress (lateral)
- Positive if excessive movement

Meniscal Injury
McMurray’s Test
Lateral meniscus:
- Flex hip and knee to 90°
- Internally rotate foot, apply varus stress, extend knee
- Pain/click = positive
Medial meniscus:
- Externally rotate foot, apply valgus stress, extend knee
- Pain/click = positive
Grind Test (Optional):
- Compress and rotate tibia over femur → meniscal damage

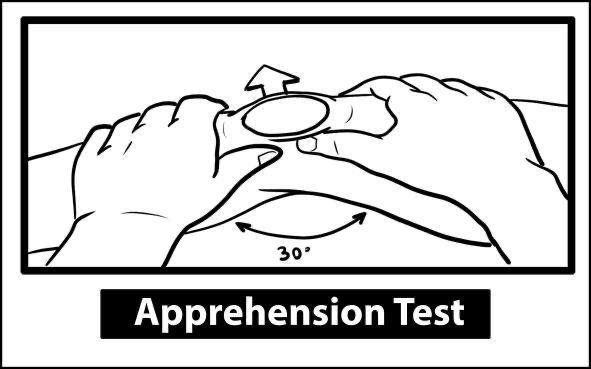
Patellar Instability
Patellar Apprehension Test
- Push patella laterally while observing for pain or guarding
→ Suggestive of patellar dislocation or patellofemoral syndrome
To Complete the Exam
- Examine hip and ankle (joint above and below)
- Neurovascular exam of the limb
Clinical Correlations
Gout
- Affects 1st MTP and lower limb joints (e.g. knee)
- Triggers: alcohol, red meat, diuretics
- Symptoms:
- Monoarthritis
- Swollen, erythematous, tender joint
- Fever in acute attacks
- Investigations:
- Uric acid, WCC
- Joint aspiration: needle-shaped, negatively birefringent crystals
- Treatment:
- Acute: NSAIDs, colchicine, steroids
- Long-term: Allopurinol (watch for rash), probenecid, pegloticase
Pseudogout
- Affects elderly; knee commonly involved
- Triggers: HHH – hyperparathyroidism, hemochromatosis, hypothyroidism
- Crystal: rhomboid, positively birefringent (calcium pyrophosphate)
- Imaging: chondrocalcinosis
- Treatment: NSAIDs, colchicine, intra-articular steroids
Septic Arthritis
- Organism: Staphylococcus aureus
- Risk factors: joint injections, prosthetic joints, immunosuppression
- Features:
- Fever, monoarthritis, erythema, effusion
- Investigations:
- Synovial fluid: purulent, ↑WCC, gram stain
- Bloods: ↑CRP, ↑WCC
- Treatment: Joint drainage + IV antibiotics
Ligament Injuries
ACL
- Mechanism: Hyperextension or twisting injury
- Audible “pop”, rapid swelling, instability
- Common in athletes
- Unhappy triad: ACL + MCL + medial meniscus
PCL
- Mechanism: Dashboard injury or hyperflexion
Collateral Ligaments
- Mechanism: Direct blow to the lateral/medial knee
- Medial (MCL) injuries more common than lateral
Meniscal Tears
- Mechanism: Twisting of flexed, weight-bearing knee
- Signs:
- Delayed effusion
- Joint line tenderness
- Locking or clicking sensation
- Quadriceps wasting
Summary – Knee Examination
The knee examination is a core OSCE skill that helps differentiate between ligamentous, meniscal, inflammatory, or degenerative knee conditions. With structured inspection, palpation, ROM testing, and special manoeuvres like McMurray’s and drawer tests, clinicians can pinpoint pathologies such as ACL tears, osteoarthritis, or gout. For a broader context, see our OSCE Prep Overview page.