Table of Contents
Overview – Gastro-Oesophageal Reflux Disease
Gastro-oesophageal reflux disease (GORD) is a common chronic condition resulting from the backflow of gastric contents into the oesophagus. It is primarily due to lower oesophageal sphincter dysfunction and can lead to mucosal inflammation, Barrett’s oesophagus, and eventually oesophageal adenocarcinoma. Early recognition and management of reflux are critical to prevent serious complications.
Definition
GORD refers to chronic regurgitation of gastric acid into the oesophagus, causing symptoms and potential complications due to mucosal damage.
Aetiology
- Primary cause: Defective lower oesophageal sphincter
- Contributing risk factors:
- Increased intra-abdominal pressure
- Hiatus hernia
- Dietary triggers: fat, alcohol, coffee, chocolate, spicy food
- Smoking
Pathogenesis
- Sphincter incompetence → reflux of acidic gastric contents
- Chronic exposure → inflammation → reflux oesophagitis
- Ongoing inflammation → metaplasia (Barrett’s oesophagus)
- Persistent injury → dysplasia → adenocarcinoma of the oesophagus
Morphology
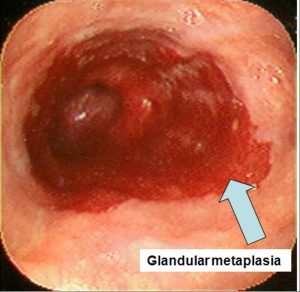
Barrett’s Oesophagus
- Endoscopic appearance:
- Upward migration of the squamo-columnar junction
- Velvety, darker pink, inflamed mucosa with irregular border
- Represents gastric metaplasia of lower oesophageal epithelium
Adenocarcinoma (Lower third)
- Endoscopic appearance:
- Wet, bulbous tumour
- Surrounding mucosa shows Barrett’s changes

Squamous Cell Carcinoma (Upper third)
- Associated with alcohol and smoking
- Endoscopic appearance:
- Dry, keratinised, ulcerated tumour

Clinical Features
- Typical symptoms:
- Heartburn (retrosternal burning)
- Dysphagia (solids → liquids)
- Complications:
- Oesophageal bleeding or perforation
- Stricture formation and obstruction
- Barrett’s oesophagus
- Malignancy (adenocarcinoma):
- Progressive dysphagia
- Weight loss, anorexia
- Aspiration risk
Investigations
- Gastroscopy + biopsy:
- Essential for identifying oesophagitis, Barrett’s, or carcinoma
- CT scan:
- Staging of oesophageal adenocarcinoma if present
Management
1. Conservative
- Lifestyle modifications:
- Raise bed-head
- Avoid meals within 3 hours of bedtime
- Reduce fat, alcohol, caffeine, spicy foods
- Weight loss
- Smoking cessation
2. Medical
- Antacids (e.g. Mylanta)
- Alginates (e.g. Aluminium salts)
- H2 receptor antagonists (e.g. Ranitidine)
- Proton-pump inhibitors (e.g. Omeprazole)
3. Surgical
- Nissen fundoplication
- Laparoscopic or open
- Gastric fundus wrapped around oesophagus to reinforce the sphincter
Summary – Gastro-Oesophageal Reflux Disease
Gastro-oesophageal reflux disease (GORD) arises due to dysfunction of the lower oesophageal sphincter, leading to chronic acid exposure. Untreated GORD can progress to Barrett’s oesophagus and eventually oesophageal adenocarcinoma. Diagnosis is confirmed via gastroscopy and biopsy, with treatment ranging from lifestyle changes to surgery. For a broader clinical overview, visit our Gastrointestinal Overview page.