Table of Contents
Overview – Anal Fistulae
Anal fistulae are abnormal epithelialised tracts that connect the anal canal to the perianal skin, usually following infection or abscess formation in the anal glands. Most cases are cryptogenic and arise due to obstruction and subsequent infection of anal crypts. Clinically, they present with pain, discharge, and in some cases, incontinence. This page outlines the aetiology, classification, symptoms, diagnosis, and treatment of anal fistulae, which are a core surgical topic in gastrointestinal medicine.
Definition
An anal fistula is a chronic abnormal tract lined with granulation tissue, connecting the anal canal to the perianal skin, usually arising from infected anal glands.
Aetiology
- Cryptogenic origin – extension of infection from obstructed anal crypts
- Often follows perianal abscess or anorectal sepsis
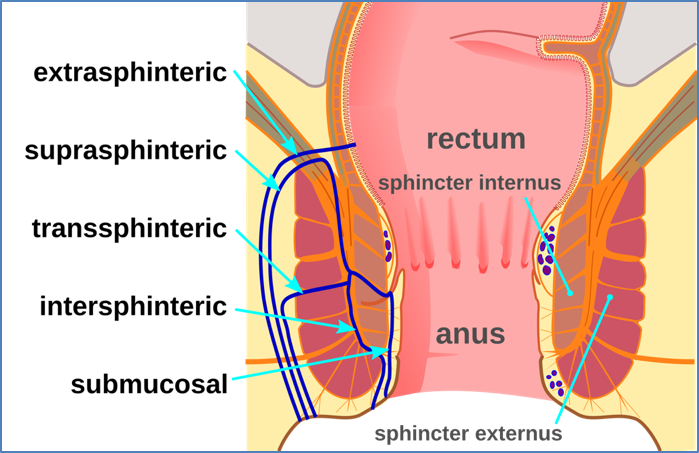
Types of Anal Fistulae
- Intersphincteric – most common
- Transsphincteric
- Suprasphincteric
- Extrasphincteric
- Submucosal
The Parks classification is commonly used to categorise fistulae based on their relationship to the sphincter muscles.
Clinical Features
- Pain – especially during or after defecation
- Purulent or faecal discharge from external opening
- Incontinence – if sphincter complex is disrupted
- Fever – may indicate ongoing infection or abscess
- Palpable external opening or cord-like tract
Investigations
- Primarily clinical diagnosis
- May include:
- Digital rectal examination
- Anoscopy
- MRI pelvis – preferred for complex or recurrent fistulae
- Endoanal ultrasound – also used to assess tract involvement
Management
- Fistulotomy – surgical unroofing of the tract (gold standard)
- Seton placement – to allow drainage while preserving sphincter function in high fistulae
- Advancement flap – for complex or recurrent cases
- Antibiotics only if there’s associated cellulitis or abscess
Complications
- Anorectal sepsis
- Recurrence
- Fistula-in-ano becoming complex
- Sphincter damage → Faecal incontinence
Summary – Anal Fistulae
Anal fistulae are chronic abnormal tracts resulting from cryptoglandular infection and are most commonly classified as intersphincteric. Diagnosis is clinical, but imaging may be used in complex cases. Surgical management, especially fistulotomy, remains the cornerstone of treatment. For a broader context, see our Gastrointestinal Overview page.