Table of Contents
Overview – Gastric Cancer
Gastric cancer is a malignant tumour arising from the epithelial lining of the stomach, most commonly in the form of adenocarcinoma. It is a leading cause of cancer-related mortality worldwide, often presenting late due to vague or absent early symptoms. The majority of cases are linked to chronic infection with Helicobacter pylori, which drives a stepwise process of gastritis, metaplasia, dysplasia, and ultimately carcinoma. This article provides a high-yield summary of the aetiology, pathogenesis, investigations, treatment and prognosis of gastric cancer for final-year medical students.
Definition
- Malignant epithelial tumour of the stomach, most commonly adenocarcinoma.
- Includes:
- Gastric adenocarcinoma (≈90%)
- MALT lymphoma
- Gastrointestinal stromal tumours (GIST)
- Carcinoid tumours (rare)
Aetiology
- H. pylori-associated metaplasia → gastric adenocarcinoma (most common pathway)
- Chronic gastritis → intestinal metaplasia → dysplasia → carcinoma
- Other causes:
- MALT lymphoma (~5%)
- GIST, carcinoid tumours, genetic syndromes (e.g. Lynch, FAP – rare)
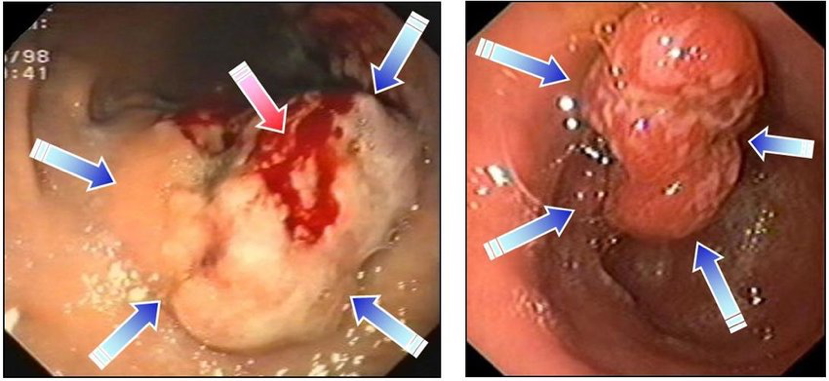
Morphology / Pathophysiology
- Fungating gastric adenocarcinoma:
- Polypoid, ulcerating lesions
- Heaped-up, rolled edges with central necrosis
- Diffuse type adenocarcinoma:
- Fibrotic infiltration of stomach wall → “leather bottle” stomach (linitis plastica)

- Progression:
- H. pylori → chronic gastritis → intestinal metaplasia → dysplasia → invasive carcinoma
Clinical Features
- Early stage:
- Often asymptomatic
- Non-specific symptoms: epigastric pain, nausea, weight loss, anaemia, haematemesis
- Late stage:
- Malignant ascites
- Jaundice (biliary or liver metastases)
- Supraclavicular node (Virchow’s node)
- Sister Mary Joseph nodule
- Brain, lung, or bone metastases
Investigations
- Gastroscopy + biopsy (gold standard for diagnosis and histological grading)
- CT scan (for staging and assessing operability)
- Tumour markers (e.g. CEA, CA 19-9) – not diagnostic, but used for monitoring
- Optional:
- PET scan – distant metastasis
- EUS (Endoscopic Ultrasound) – locoregional staging
Management
- Surgical:
- Total gastrectomy or subtotal gastrectomy
- Oesophagojejunostomy reconstruction
- Sentinel node resection, ± splenectomy if involved
- Adjunct therapies:
- Chemotherapy (adjuvant or palliative)
- Radiotherapy (palliative)
- Targeted therapy in HER2+ cases (e.g. trastuzumab)
- Nutritional support: essential pre- and post-op
Prognosis
- Typically poor due to late presentation
- <30% 5-year survival post-surgery
- Prognosis depends on stage at diagnosis and resectability
Differential Diagnosis
- Peptic ulcer disease
- Gastritis
- Functional dyspepsia
- GIST
- MALT lymphoma
Summary – Gastric Cancer
Gastric cancer is a malignant tumour of the stomach, most often caused by Helicobacter pylori-induced metaplasia and chronic inflammation. The disease is frequently asymptomatic in early stages and often presents late with haematemesis, weight loss, anaemia, or metastatic signs. Diagnosis is confirmed by gastroscopy and biopsy, with staging via CT. Management involves surgical resection with or without adjuvant therapy, but overall prognosis remains poor. For a broader context, see our Gastrointestinal Overview page.