Table of Contents
Overview – Zollinger-Ellison Syndrome
Zollinger-Ellison Syndrome (ZES) is a rare but clinically significant cause of treatment-resistant peptic ulcer disease. It results from gastrin-secreting neuroendocrine tumours (gastrinomas), typically located in the pancreas or duodenum. These tumours drive excessive gastric acid secretion, leading to recurrent, severe ulcers and gastrointestinal symptoms. Recognising ZES is crucial in cases of refractory peptic ulcers, especially in younger patients or those with ulcers in atypical locations. This article outlines the key diagnostic features, complications, and treatment of Zollinger-Ellison Syndrome for final-year medical students.
Definition
- A rare condition caused by gastrin-secreting neuroendocrine tumours (gastrinomas).
- Results in hypergastrinaemia → excessive gastric acid production → peptic ulcer disease.
Aetiology
- Gastrinomas most commonly occur in:
- Duodenum (~45%)
- Pancreas (~25%)
- Stomach (rare)
- Can occur sporadically or as part of Multiple Endocrine Neoplasia type 1 (MEN1).
Pathophysiology
- Gastrinoma secretes excess gastrin:
- → stimulates parietal cells → ↑ HCl secretion
- → ↑ pepsin secretion (from chief cells)
- → treatment-resistant peptic ulcers (both gastric and duodenal)
- → intestinal mucosal damage and enzyme inactivation
- Ulcers may be multiple, recurrent, or located in atypical sites (e.g. jejunum).
Clinical Features
- Abdominal pain
- Dyspepsia
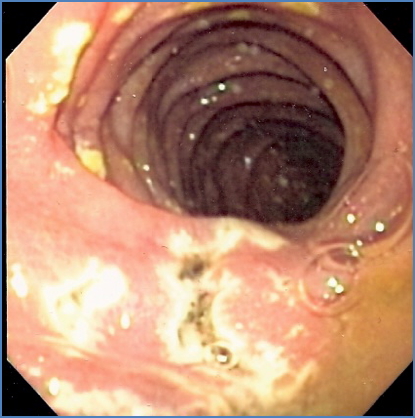
- Recurrent peptic ulcer disease (PUD):
- Often with haematemesis or melena
- May result in ulcer perforation → peritonitis, shock
- Chronic diarrhoea:
- Due to acid-induced inactivation of pancreatic enzymes (e.g. lipase)
- May be the presenting symptom in some cases
Investigations
- Fasting serum gastrin (screening test):
- Elevated levels (>10x normal) suggest ZES
- Endoscopic ultrasound:
- Detects pancreatic or duodenal masses
- CT or MRI scan:
- Staging and localisation of tumour
- Additional:
- Secretin stimulation test (if gastrin borderline)
- Somatostatin receptor scintigraphy (Octreotide scan)
Management
- Medical:
- Proton pump inhibitors (PPIs) – Omeprazole:
- First-line to control hyperacidity
- Proton pump inhibitors (PPIs) – Omeprazole:
- Surgical:
- Resection of the gastrinoma (if localised)
- 80% 5-year survival if successfully removed
- Advanced/metastatic:
- May require chemotherapy or somatostatin analogues
Complications
- Malignant potential:
- ~60% of gastrinomas are malignant, often with liver metastases
- Recurrent or intractable ulcers
- Gastrointestinal bleeding
- Perforation → peritonitis
- Nutritional deficiency from chronic diarrhoea
Differential Diagnosis
- Peptic ulcer disease (common causes: NSAIDs, H. pylori)
- Gastritis
- Crohn’s disease (if chronic diarrhoea)
- Pancreatic insufficiency
Summary – Zollinger-Ellison Syndrome
Zollinger-Ellison Syndrome is a rare cause of severe peptic ulcer disease, driven by gastrinomas that stimulate excessive gastric acid secretion. It presents with abdominal pain, chronic diarrhoea, and treatment-resistant ulcers. Diagnosis is made by elevated serum gastrin levels and imaging, and management involves PPIs and possible surgical resection. Recognising ZES is essential for managing unexplained or refractory PUD. For more GI conditions, visit our Gastrointestinal Overview page.