Table of Contents
Overview – Hypophosphatemic Rickets
Hypophosphatemic rickets is a genetic disorder that impairs phosphate reabsorption in the kidneys, resulting in soft, weak bones and skeletal deformities. Unlike classical rickets caused by vitamin D deficiency, this subtype is often due to mutations affecting renal phosphate handling, most commonly via the PHEX gene. Early recognition and management are essential to minimise deformities and support normal growth and development.
Definition
Hypophosphatemic rickets is a form of rickets caused by inadequate phosphate levels due to renal phosphate wasting, often stemming from genetic mutations rather than vitamin D deficiency.
Aetiology
General Causes of Rickets:
- Vitamin D Deficiency:
- Inadequate dietary intake
- Limited sunlight exposure
- Malabsorption syndromes (affecting fat-soluble vitamins: A, D, E, K)
- Disrupted Vitamin D Metabolism:
- Liver or renal dysfunction
- Genetic defects in vitamin D metabolism
- End-organ resistance to vitamin D
- Abnormal Renal Phosphate Handling:
- Genetic hypophosphatemic rickets (e.g. PHEX mutation)
- Tumour-induced osteomalacia (paraneoplastic syndrome)
Genetics of Hereditary Hypophosphatemic Rickets:
- Inheritance pattern: X-linked dominant (most common), though rare recessive forms exist
- Can be inherited from either parent
- Affected fathers cannot transmit to sons
- Affected phenotypes:
- Heterozygous (females)
- Homozygous (females)
- Hemizygous (males)
- Females have higher statistical chance of inheritance due to dual X-chromosome presence
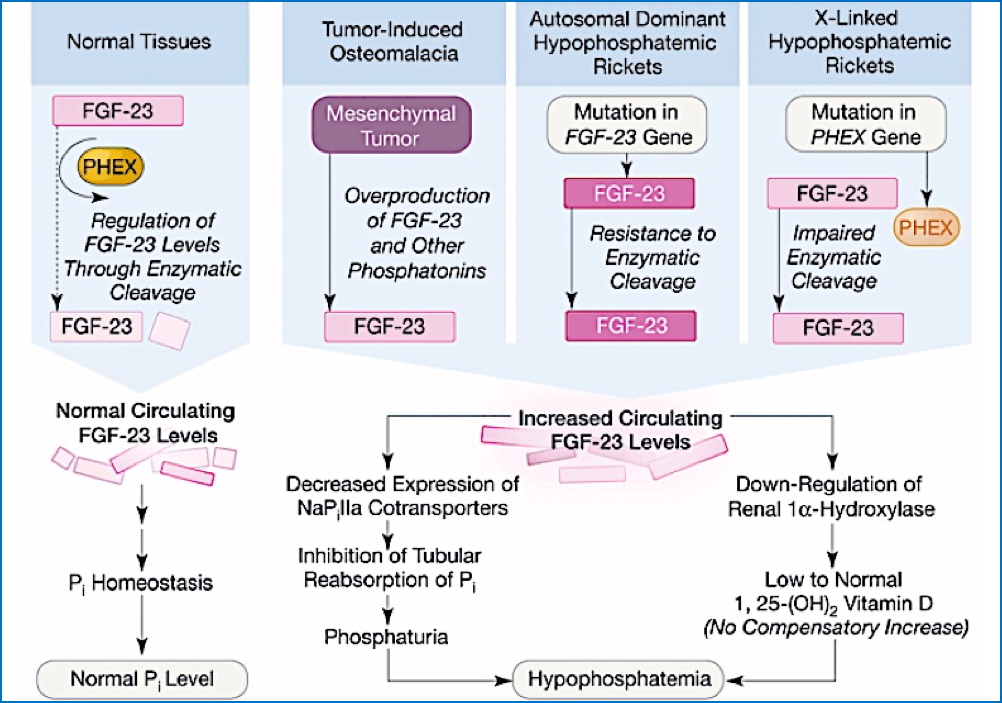
Pathophysiology
- Most often caused by a mutation in the PHEX gene, which normally suppresses phosphate-wasting
- The mutation causes a gain-of-function, leading to excess fibroblast growth factor 23 (FGF23) activity
- This results in:
→ ↓ Renal phosphate reabsorption
→ Chronic hypophosphataemia
→ Impaired bone mineralisation
→ Skeletal deformities and pain
Clinical Features
- Bone and joint pain
- Bowing of the legs
- Short stature
- Soft bones (osteomalacia)
- Poor bone growth and delayed milestones
- Developmental abnormalities
- Skeletal deformities become more noticeable with age
Investigations
- Serum biochemistry:
- ↓ Serum phosphate
- Normal or ↑ Alkaline phosphatase
- Normal serum calcium
- Low/normal 1,25-dihydroxyvitamin D
- Genetic testing for PHEX mutations
- Renal phosphate handling studies
Management
- Medical Therapy:
- Calcitriol (active vitamin D: 1,25-dihydroxyvitamin D)
- Oral phosphate supplements
- Monitoring:
- Regular assessment of growth, serum phosphate, and vitamin D levels
- Orthopaedic Support:
- Physiotherapy
- Surgical correction for severe deformities
Prognosis
- With timely diagnosis and adequate treatment, children can achieve near-normal growth and good quality of life
- Permanent skeletal deformities may persist if treatment is delayed
- Lifespan is generally unaffected with appropriate management
Summary – Hypophosphatemic Rickets
Hypophosphatemic rickets is an inherited disorder characterised by impaired phosphate reabsorption in the kidneys, resulting in soft, painful bones and skeletal deformities. It is most commonly X-linked dominant, caused by mutations in the PHEX gene. Early diagnosis and treatment with phosphate and calcitriol can improve outcomes significantly. For a broader context, see our Genetics & Cancer Overview page.