Table of Contents
Overview – Muscular Dystrophies
Muscular dystrophies are a group of inherited disorders characterised by progressive muscle weakness and degeneration. The most common forms, Duchenne muscular dystrophy (DMD) and Becker muscular dystrophy (BMD), are caused by mutations in the dystrophin gene and follow an X-linked recessive inheritance pattern. Early diagnosis and supportive care are vital to prolong mobility and monitor for cardiac and respiratory complications.
Definition
Muscular dystrophies are genetic conditions that lead to progressive muscle wasting and weakness, due to abnormalities in muscle structural proteins, most notably dystrophin.
Aetiology
- Genetic Basis:
- Inherited in an X-linked recessive pattern
- Caused by mutations in the dystrophin gene, the largest known human gene
- The gene mutation leads to reduced or absent dystrophin protein, a critical membrane-stabilising protein in muscle fibres
- Dystrophin Function:
- Located beneath the sarcolemma (muscle cell membrane) of skeletal and cardiac muscle
- Plays a key role in protecting muscle fibres from injury during contraction
- Absence or malfunction leads to membrane instability → inflammation → fibrosis → muscle degeneration
Types of Muscular Dystrophy
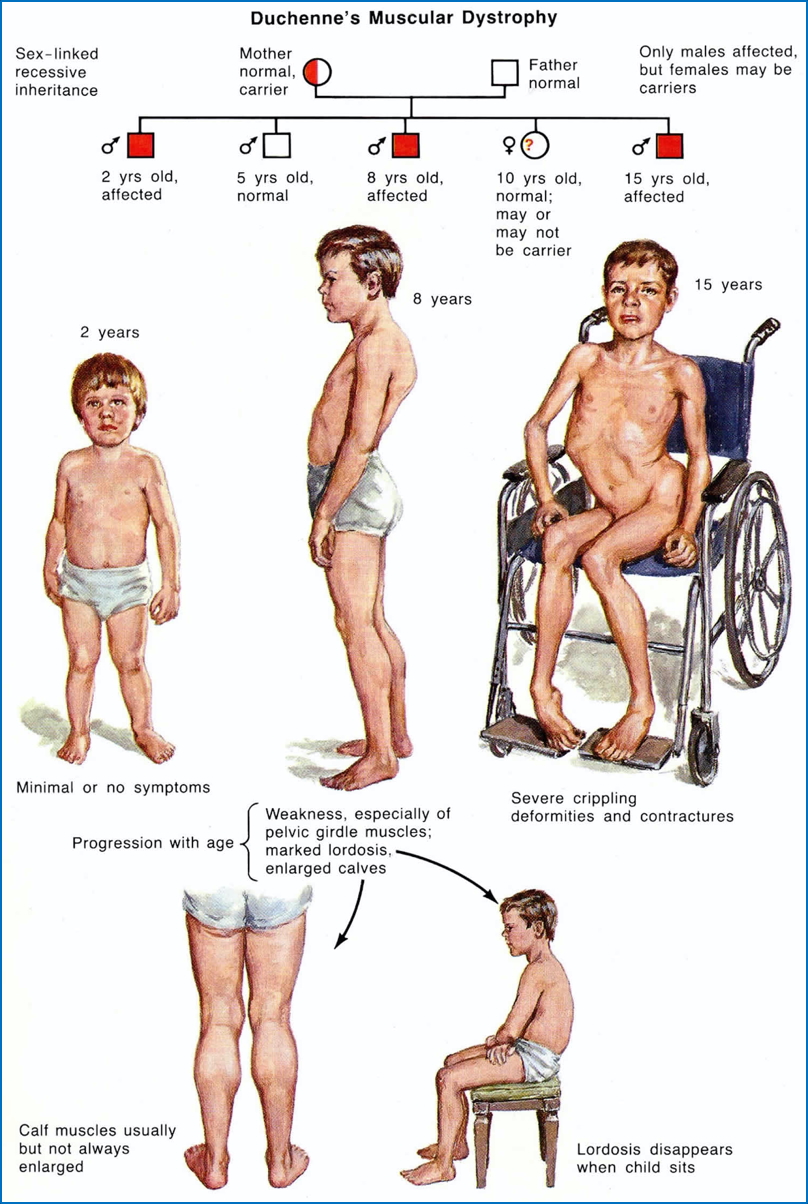
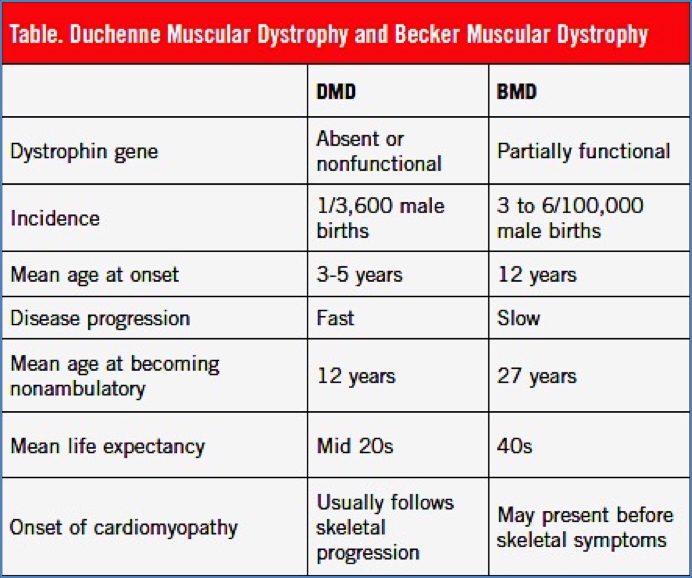
Duchenne Muscular Dystrophy (DMD)
- Most severe and common form of X-linked muscular dystrophy
- Onset: Early childhood (usually before age 5)
- Clinical Features:
- Gower’s manoeuvre (uses hands to climb up legs when rising from floor)
- Waddling gait
- Calf pseudohypertrophy (enlarged calves due to fat and connective tissue)
- Scoliosis
- Wheelchair dependence by early teens
- Reduced pulmonary function by ~20 years
- Mortality due to:
- Respiratory failure
- Cardiac failure (dilated cardiomyopathy)
- Females:
- Carriers usually asymptomatic due to random X-inactivation balancing
- However, some may develop cardiomyopathy and require regular cardiac check-ups

2. https://healthjade.net/duchenne-muscular-dystrophy/
Becker Muscular Dystrophy (BMD)
- Milder phenotype of dystrophinopathy
- Onset: Between 5–15 years of age
- Clinical Features:
- Slower progression than DMD
- Immobility ~20 years after symptom onset
- Calf hypertrophy
- Toe-walking
- Longer preservation of ambulation and life expectancy than DMD

Investigations
- Creatine Kinase (CK): Elevated levels suggest muscle breakdown
- Genetic Testing: Confirms mutations in the dystrophin gene
- Muscle Biopsy: Reveals absent or reduced dystrophin expression
- Cardiac Evaluation: Echocardiography and ECG for cardiomyopathy
- Respiratory Function Tests: Monitor for decline
Management
- Pharmacological:
- Corticosteroids (e.g. prednisone) to slow muscle degeneration
- Newer agents: exon-skipping therapies, gene therapy trials underway
- Supportive Care:
- Physiotherapy and stretching to reduce contractures
- Occupational therapy and assistive devices
- Respiratory support (e.g. BiPAP in advanced cases)
- Cardiac medications (ACE inhibitors, beta-blockers)
- Monitoring for female carriers is essential, particularly for cardiac involvement
Prognosis
- Duchenne MD:
- Rapidly progressive
- Life expectancy ~20–30 years with optimal care
- Becker MD:
- Slower progression
- Survival into mid-late adulthood is possible
Summary – Muscular Dystrophies
Muscular dystrophies, especially Duchenne and Becker types, are X-linked recessive disorders due to mutations in the dystrophin gene. Duchenne presents early and progresses rapidly, while Becker is milder with later onset. Early multidisciplinary care improves quality of life and survival. For a broader context, see our Genetics & Cancer Overview page.