Table of Contents
Overview – Systemic Lupus Erythematosus
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease that affects multiple organ systems and is characterised by the production of numerous antinuclear antibodies. SLE disproportionately affects women and can present with diverse manifestations, including skin rashes, arthritis, nephritis, and haematological abnormalities. The immune system in SLE attacks self-tissues directly or via immune complex deposition, leading to inflammation and tissue damage. Accurate diagnosis requires a combination of clinical criteria and immunological testing.
Definition
Systemic lupus erythematosus (SLE) is a chronic, multisystem autoimmune disease defined by:
- Widespread production of antinuclear antibodies (ANA) including:
- Anti-dsDNA
- Anti-ribonucleoprotein
- Anti-histone antibodies
- Immune complex formation and deposition in tissues (especially the skin, joints, kidneys, and CNS)
- Female predominance: F:M ratio ≈ 10:1
Pathogenesis
SLE results from a loss of self-tolerance and epitope spreading, involving the following steps:
- Apoptotic Cell Debris: Damaged or dying cells release nuclear material into the extracellular space
- B-Cell Activation: Histone-specific B-cells bind nuclear antigens and present them to autoreactive CD4+ T-helper cells
- T-Cell Help: Histone-specific T-cells provide help to DNA-specific B-cells
- Autoantibody Production: Anti-DNA antibodies form immune complexes with nucleosomes and complement (notably C3)
- Tissue Deposition: Immune complexes deposit in organs, particularly the kidneys → glomerulonephritis
- Genetic Factors:
- Genetic predisposition contributes
- Fas ligand deficiency → defective clearance of autoreactive T-cells

Clinical Manifestations
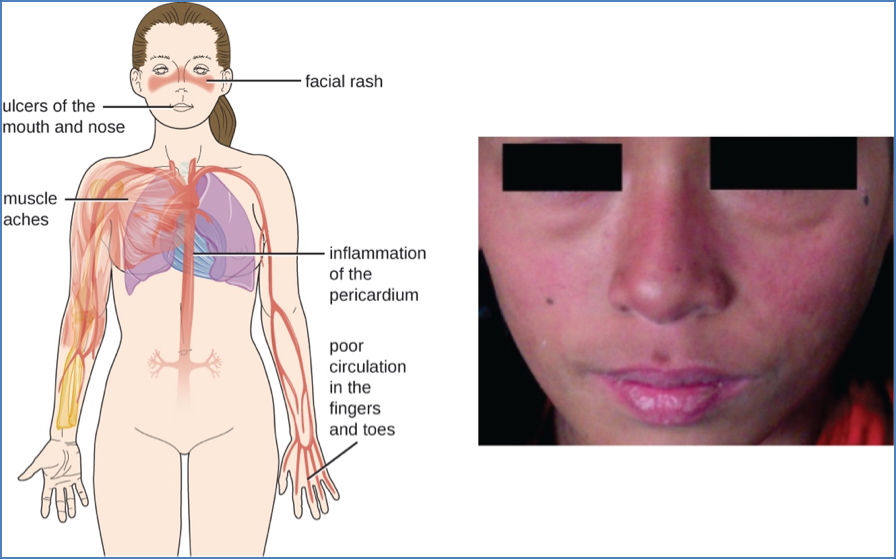
SLE can affect nearly every organ system. Common manifestations include:
- Skin:
- Malar rash (butterfly rash)
- Discoid rash
- Photosensitivity
- Mucosa:
- Oral and nasal ulcers
- Musculoskeletal:
- Non-erosive arthritis (commonly small joints)
- Renal:
- Glomerulonephritis
- Proteinuria
- Cellular casts
- Haematological:
- Haemolytic anaemia
- Thrombocytopenia
- Leukopenia
- Neurological:
- Seizures
- Psychosis
- Cardiopulmonary:
- Pleuritis
- Pericarditis
- Pericardial/pleural effusions
Diagnosis
Immunological Tests
- Antinuclear Antibody (ANA)
- Present in ~95% of cases
- Sensitive but not specific for SLE
- Extractable Nuclear Antigen (ENA) Panel
- Identifies specific antibodies such as anti-dsDNA, anti-Sm, anti-RNP
- Helps confirm the diagnosis when ANA is positive
Clinical Diagnostic Criteria (Selected ACR Criteria)
- Malar rash
- Discoid rash
- Photosensitivity
- Oral ulcers
- Non-erosive arthritis
- Serositis (pleuritis or pericarditis)
- Renal disorder (proteinuria, cellular casts)
- Neurologic disorder (seizures, psychosis)
- Haematologic disorder (anaemia, leukopenia, thrombocytopenia)
- Positive ANA or specific autoantibodies
Summary – Systemic Lupus Erythematosus
Systemic lupus erythematosus is a complex autoimmune disorder defined by autoantibody production and multi-organ involvement, particularly affecting the skin, joints, kidneys, and blood. Diagnosis involves clinical findings and immunological markers such as ANA and ENA. The underlying pathogenesis involves loss of immune tolerance, epitope spreading, and immune complex deposition. For more foundational concepts, see our Immune & Rheumatology Overview page.