Table of Contents
Overview – Intrauterine Growth Anomalies
Intrauterine growth anomalies refer to deviations from normal fetal growth patterns during gestation, most commonly presenting as intrauterine growth restriction (IUGR) or fetal macrosomia. Intrauterine growth restriction is defined as a fetal weight below the 10th percentile for gestational age, while macrosomia refers to excessive fetal growth, typically above the 90th percentile or >4000g. These conditions have opposing pathophysiology but both carry significant perinatal risks and require careful antenatal surveillance and delivery planning.
Intrauterine Growth Restriction
Definition
- Birth weight <10th percentile for gestational age
- OR <2500g at term
Aetiology
Maternal Causes
- Malnutrition
- Smoking, alcohol, drug use
- Hypertension
- Diabetes mellitus
- Systemic lupus erythematosus (SLE)
Placental Causes
- Placental insufficiency
- Multiple gestation
- Prolonged pregnancy
Fetal Causes
- Congenital or chromosomal abnormalities
- TORCH infections:
- Toxoplasmosis
- Others (e.g. syphilis)
- Rubella
- Cytomegalovirus (CMV)
- Herpes simplex virus (HSV)
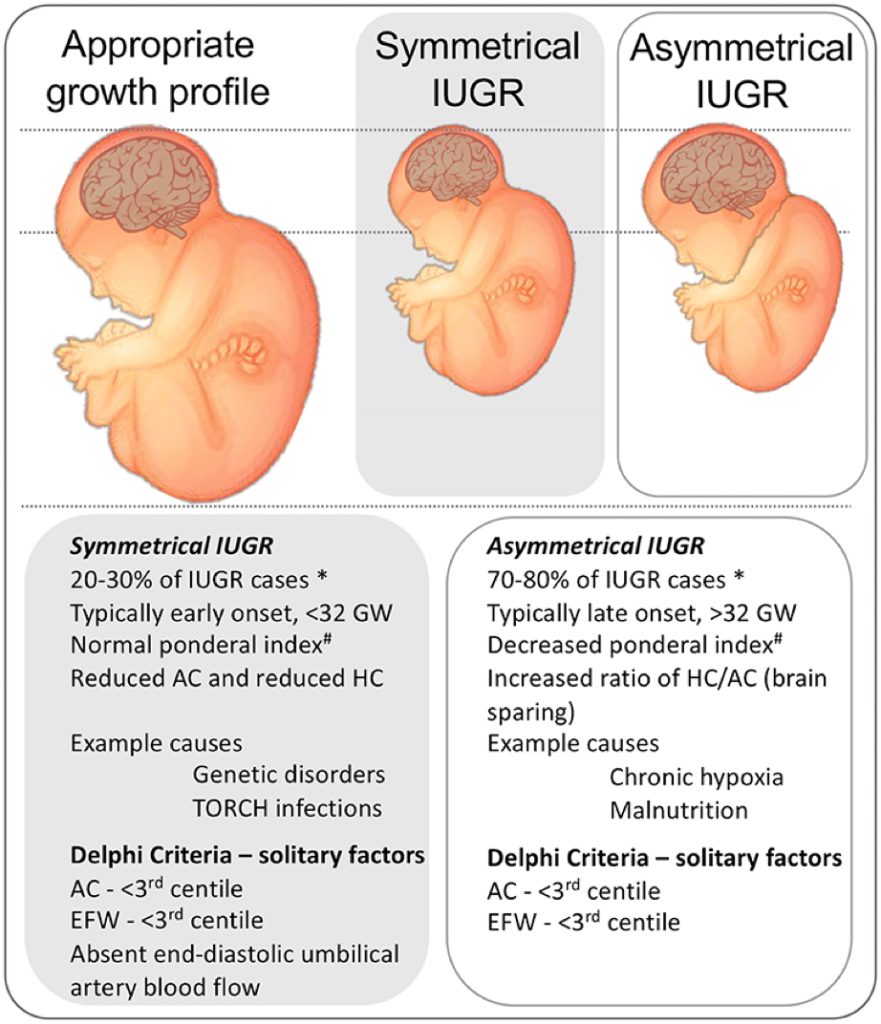
Clinical Features
Symmetric IUGR
- Head and abdominal growth equally reduced
- Normal Head:Abdomen ratio:
- 1 at <32 weeks
- ≈1 at 32–34 weeks
- <1 after 34 weeks
- Common in congenital anomalies or infections
Asymmetric IUGR
- Abdominal circumference reduced more than head circumference
- Increased Head:Abdomen ratio
- Suggests placental insufficiency
Investigations
- Fundal height measurement
- Fetal ultrasound (head/abdominal circumference, femur length, amniotic fluid)
- Umbilical artery Doppler
Management
- Modify maternal risk factors
- Bed rest in left lateral position
- Determine timing of delivery based on risk-benefit balance
- Consider caesarean delivery if fetal distress or severe IUGR
Complications
- Stillbirth
- Neonatal hypoxia and hypoglycaemia
- Neurodevelopmental delay
Macrosomia
Definition
- Birth weight >90th percentile for gestational age
- OR >4000g at any time
Aetiology
- Maternal obesity
- Gestational diabetes mellitus
- Prolonged gestation
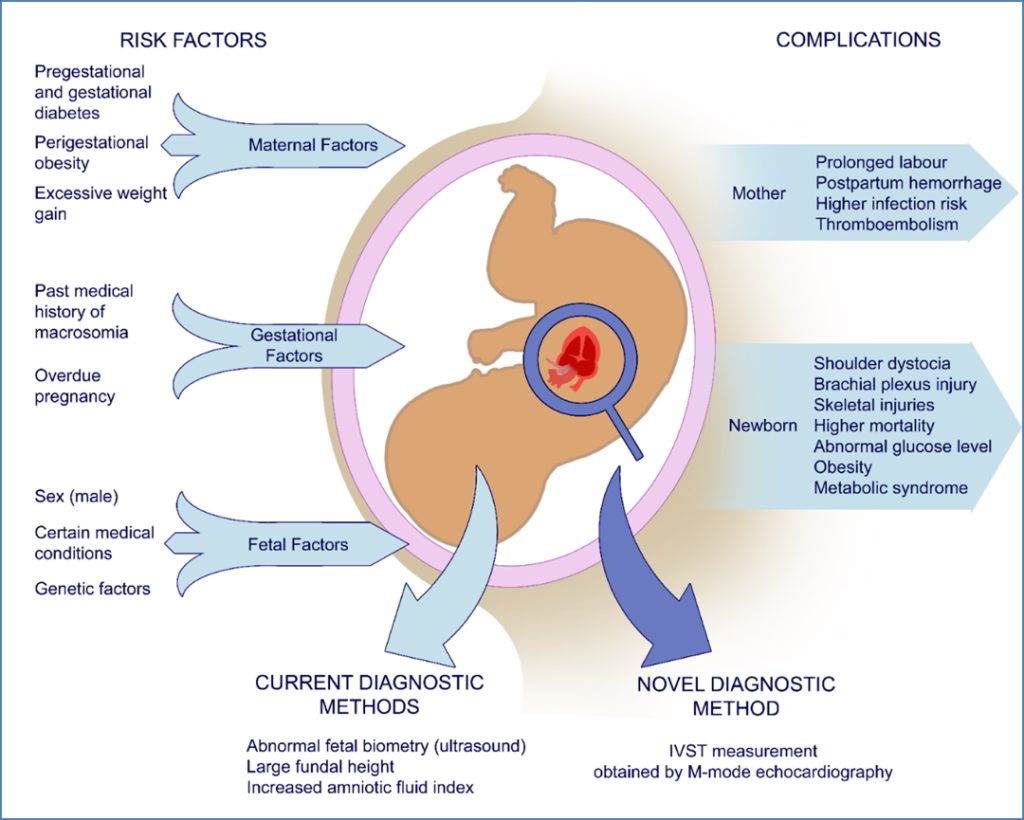
Clinical Features
- Increased risk of:
- Shoulder dystocia
- Birth trauma (clavicle fracture, brachial plexus injury)
- Polyhydramnios
- Measurement ratios suggestive of macrosomia:
- Head Circumference:Abdominal Circumference <10th percentile
- Femur Length:Abdominal Circumference <20th percentile

Management
- Elective caesarean if estimated fetal weight >5000g (non-diabetic mother) or >4500g (diabetic mother)
- Monitor closely for delivery complications
Prognosis
- Increased perinatal morbidity and mortality
- Risk of postpartum complications (e.g. maternal haemorrhage)
Summary – Intrauterine Growth Anomalies
Intrauterine growth anomalies encompass both intrauterine growth restriction (IUGR) and macrosomia, representing opposite ends of the fetal growth spectrum. IUGR reflects growth failure and is often linked to placental insufficiency or infections, whereas macrosomia is associated with maternal diabetes and obesity. Early recognition and appropriate management are essential to reduce perinatal risks. For more information, visit our Obstetrics Overview page.