Table of Contents
Overview – Minimal Change Disease
Minimal Change Disease (MCD) is the most common cause of nephrotic syndrome in children aged 1–8 years. Also known as “Nil Disease” or “Foot Process Disease”, MCD is characterised by a dramatic loss of protein in the urine (selective proteinuria), often following a recent upper respiratory tract infection or immunisation. Despite significant proteinuria and oedema, renal function typically remains preserved, and most cases respond excellently to corticosteroid therapy. Understanding MCD is essential for differentiating paediatric nephrotic syndromes and initiating early, effective treatment.
Definition
Minimal Change Disease is a glomerular disorder marked by:
- Sudden onset of nephrotic syndrome, particularly in children
- Histologically normal-appearing glomeruli under light microscopy, but with effacement of podocyte foot processes on electron microscopy
- Selective proteinuria (primarily albumin loss)
Aetiology
- Idiopathic (most common)
- Post-infectious (e.g. following URTI)
- Post-immunisation
- Drug-induced: NSAIDs are a known trigger
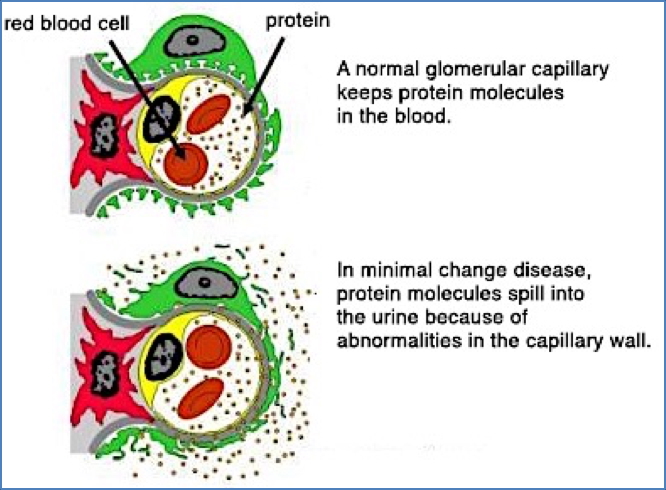
Pathophysiology
- T-cell–derived cytokines damage podocytes
- → Effacement (flattening) of podocyte foot processes
- → Disruption of the glomerular filtration barrier
- → Selective protein loss (mainly albumin) in urine
- → Nephrotic syndrome develops with oedema and hypoalbuminaemia
Importantly, there is no immune complex deposition or glomerular inflammation—making it unique among glomerulopathies.

Clinical Features
- Most commonly affects children aged 1–8 years
- Classic presentation:
- Sudden onset oedema (especially periorbital)
- Polyuria
- Frothy urine due to proteinuria
- Often follows recent URTI or vaccination
- Systemically well aside from oedema
- Prognosis:
- Excellent in children: <70% experience spontaneous remission
- A minority may progress to Focal Segmental Glomerulosclerosis (FSGS)
Investigations
- Urinalysis:
- +++ Proteinuria (>3.5g/day)
- No haematuria or casts
- Serum biochemistry:
- ↓ Serum albumin
- ↑ Serum cholesterol (hyperlipidaemia)
- Renal biopsy:
- Often avoided in classic paediatric cases
- Shows normal glomeruli on light microscopy
- Electron microscopy reveals podocyte effacement
Management
- First-line: Oral Prednisone
- Most patients respond rapidly within 1–2 weeks
- Supportive treatment:
- Diuretics for oedema (e.g. frusemide)
- Salt and fluid restriction
- Monitor urine protein levels and relapse risk
- Relapsing cases:
- May require immunosuppressants (e.g. cyclophosphamide, calcineurin inhibitors)
Complications
- Relapse: Common but usually steroid-responsive
- Progression to FSGS (especially in steroid-resistant cases)
- Infection risk: Due to loss of immunoglobulins in urine
- Thromboembolism: Due to loss of antithrombin-III in urine
Differential Diagnosis
- Focal Segmental Glomerulosclerosis (FSGS)
- Membranous nephropathy
- Diabetic nephropathy
- Congenital nephrotic syndrome (in neonates)
Summary – Minimal Change Disease
Minimal Change Disease is the leading cause of nephrotic syndrome in children, presenting with selective proteinuria, oedema, and preserved renal function. Prompt recognition and corticosteroid therapy often lead to full remission. Understanding MCD is key in paediatric renal practice. For more renal pathology topics, see our Renal Overview page.