Table of Contents
Overview – Menorrhagia
Menorrhagia is defined as excessive menstrual bleeding, typically >80 mL per cycle, though this is difficult to measure directly. It affects up to 1 in 5 women, with a range of causes from hormonal imbalances to structural uterine pathology. Menorrhagia can significantly impair quality of life and often presents with symptoms of iron deficiency anaemia.
Definition
Heavy menstrual bleeding lasting longer than 7 days and/or requiring pad/tampon changes more than once every 4 hours.
Clinical Presentation
- Bleeding lasting >7 days (normal ≈ 5 days)
- Heavy flow: needing frequent pad/tampon changes (more than every 4 hrs)
- Flooding: blood not contained by pads/tampons
- Large clots (>3cm diameter; small stringy clots are normal)
- Symptoms of iron deficiency anaemia (e.g. fatigue, pallor, dizziness)
Common Causes
- Dysfunctional Uterine Bleeding (DUB)
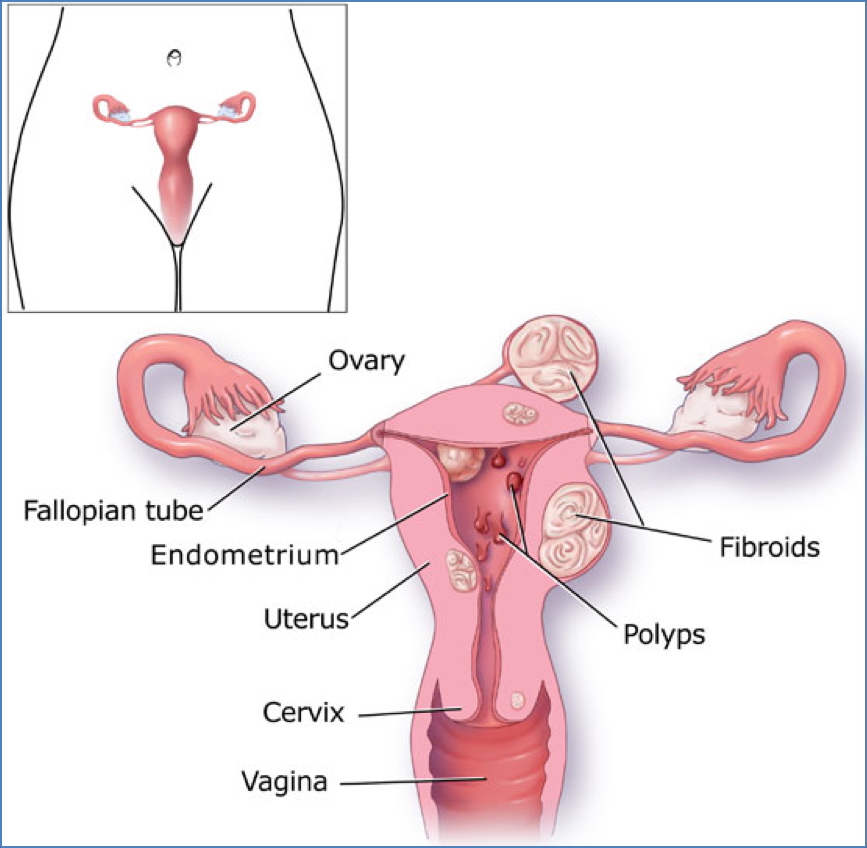
- Uterine fibroids
- Endometrial hyperplasia
- Adenomyosis
Other Less-Common Causes
- Endometrial cancer
- Bleeding disorders (e.g. Von Willebrand disease)
- Hyperthyroidism
- IUD-related bleeding
Investigations
1. Speculum & Bimanual Vaginal Examination
- Identify cervical or vaginal lesions, uterine size, or masses
2. Transvaginal Ultrasound
- No abnormalities → Suggests Dysfunctional Uterine Bleeding (DUB)
- Well-defined myometrial mass → Suggests fibroid
- Endometrial thickening → Suggests endometrial hyperplasia
- Myometrial thickening → Suggests adenomyosis
3. Endometrial Sampling
- Pipelle biopsy or hysteroscopy for histological confirmation
4. Laparoscopy
- Considered in patients with menorrhagia plus infertility, pelvic pain, or suspected ovarian pathology
Management
Medical (First-line)
1. Progesterone-Only IUD or Tablets (Most Effective)
- Mechanism: Suppresses endometrial proliferation → lighter periods
- Efficacy: ~95% reduction in blood loss
- Duration: Effective for up to 5 years
- Side Effects: Irregular spotting in first few months
2. Combined Oral Contraceptive Pill
- Reduces blood loss by ~30%
- Additional benefit: contraception
3. NSAIDs (e.g. ibuprofen, aspirin)
- Decrease prostaglandin-mediated blood loss and reduce dysmenorrhoea
- ~30% reduction in blood loss
4. Iron Supplementation
- For correction of anaemia due to chronic blood loss
Surgical (Reserved for women not planning pregnancy)
1. Endometrial Ablation
- Hysteroscopic destruction of endometrial lining
- ~85% effective
- Up to 40% may become infertile
2. Hysterectomy
- Definitive cure
- 100% effective
- Results in permanent infertility
- Routes: abdominal, vaginal, or laparoscopic
Dysfunctional Uterine Bleeding (DUB)
Aetiology
- Excess oestrogen → unopposed endometrial proliferation
Diagnosis
- Diagnosis of exclusion (no structural or hormonal cause identified)
Management
- Hormonal contraceptives
- Aim to regulate or eliminate menstruation
Summary – Menorrhagia
Menorrhagia, or heavy menstrual bleeding, is a common gynaecological complaint with a wide differential. Diagnosis involves ruling out structural pathology via ultrasound and endometrial sampling. First-line treatment is hormonal therapy, particularly progesterone IUDs, with surgery reserved for non-fertility-seeking patients. See our Reproductive Health page for more related content.