Table of Contents
Overview – Bronchiolitis
Bronchiolitis is a common lower respiratory tract infection in infants and young children, characterised by inflammation and obstruction of the small airways (bronchioles), most commonly caused by Respiratory Syncytial Virus (RSV). It frequently follows a viral upper respiratory prodrome and can lead to respiratory distress, wheezing, and feeding difficulties. While most cases are mild and self-limiting, hospitalisation may be required for infants with hypoxia, severe tachypnoea, or poor feeding.
Definition
Bronchiolitis refers to inflammation and obstruction of the bronchioles, usually caused by viral infection, primarily affecting infants under 2 years of age.
Aetiology
Viral Causes (Most Common)
- Respiratory Syncytial Virus (RSV) – >50% of cases
- Parainfluenza
- Influenza
- Rhinovirus
- Adenovirus
Rare Atypical Causes
- Mycoplasma pneumoniae
Pathogenesis of Bronchiolitis
Viral infection of the epithelial cells in bronchioles → inflammation, oedema, mucus production, and necrosis → narrowing of airways → air trapping and impaired gas exchange. Infants are especially vulnerable due to small airway calibre and limited respiratory reserve.

Clinical Features of Bronchiolitis
General Presentation
- Common in children <2 years; peak incidence at 2–6 months
- Often follows a 1–3 day upper respiratory prodrome
Respiratory Signs
- Cough
- Wheezing
- Tachypnoea
- Tachycardia
- Signs of increased work of breathing:
- Intercostal and subcostal recessions
- Tracheal tug
- Supraclavicular indrawing
- Nasal flaring
- Rib flaring
Systemic Signs
- Fever
- Irritability
- Poor feeding/dehydration
Investigations
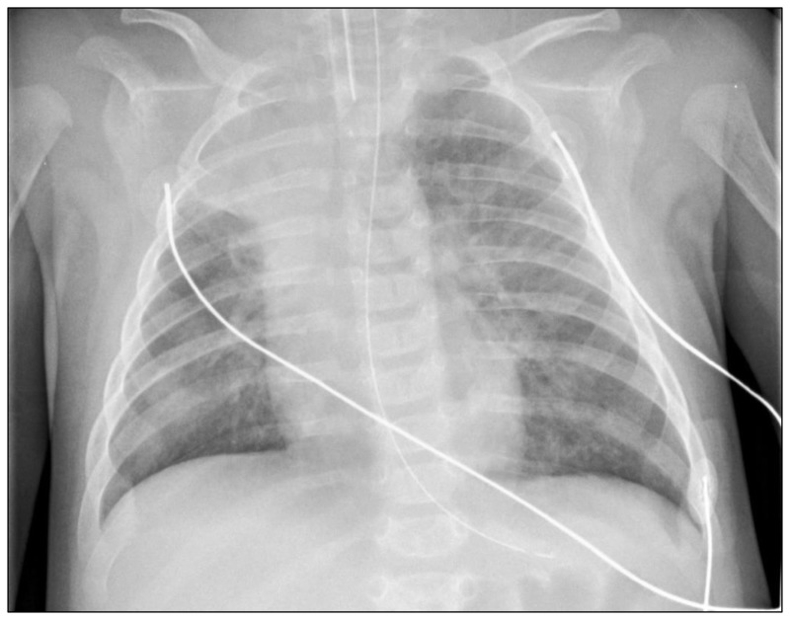
- Chest X-Ray:
- Hyperinflation (air trapping)
- Peribronchial thickening
- Atelectasis
- Increased linear markings
- Nasopharyngeal Aspirate (NPA): PCR to detect viral cause
- FBC: Lymphocytosis may be present
Indications for Hospital Admission
- SpO₂ <92% on room air
- Respiratory rate >60–70/min in infants
- Moderate to severe respiratory distress despite bronchodilator
- Age <6 months
- Apnoea or cyanotic episodes
- Inability to feed (poor oral intake or dehydration)
Management
Supportive Therapy (Mainstay)
- Fluid rehydration (oral or IV)
- Paracetamol for fever
- Humidified oxygen
- Gentle nasal suctioning (if obstructive secretions)
Bronchodilators
- Salbutamol (Ventolin) trial may be attempted, but response is variable and often minimal
Advanced Management
- Intubation and ventilation if:
- Severe respiratory distress
- Persistent hypoxaemia
- Rising CO₂ (impending respiratory failure)

Complications
- Respiratory failure (requiring ventilation)
- Apnoea in very young infants
- Secondary bacterial infection (rare)
- Recurrent wheeze or asthma later in childhood (in some cases)
Summary – Bronchiolitis
Bronchiolitis is a viral lower respiratory tract infection predominantly affecting infants and young children, typically caused by RSV. While most cases are self-limiting, some children develop significant respiratory distress requiring hospitalisation. Management is largely supportive, with a focus on oxygenation, hydration, and monitoring. For broader context, visit our Respiratory Overview page.