Table of Contents
Overview – Sarcoidosis
Sarcoidosis is a multisystem granulomatous disorder of unknown aetiology that most commonly affects the lungs and intrathoracic lymph nodes. It is characterised by the presence of non-caseating granulomas, which may lead to fibrosis and organ dysfunction. Although it often resolves spontaneously, some cases progress to chronic disease, especially with pulmonary involvement.
Definition
A systemic inflammatory disorder characterised by the formation of non-caseating granulomas in affected organs, most commonly the lungs.
Aetiology
- Idiopathic
- Likely immune-mediated with possible contributions from:
- Environmental exposures (e.g. dusts, moulds)
- Infectious triggers (e.g. mycobacteria, viruses)
- Genetic predisposition (family clustering in some populations)
Pathogenesis
- Activation of alveolar macrophages and CD4+ T-helper cells
- → Cytokine release (especially IL-2 and IFN-γ)
- → Formation of non-caseating granulomas
- Granulomas may resolve or progress to fibrosis, depending on immune regulation and persistence of triggering antigens
Morphology
- Histology:
- Non-caseating granulomas composed of tightly clustered epithelioid macrophages and multinucleated giant cells
- Absence of central necrosis (differentiating from TB)
- Organ Distribution:
- Lungs (most common)
- Hilar and mediastinal lymph nodes
- Skin (e.g. erythema nodosum)
- Eyes, liver, kidneys, CNS, heart
- Imaging:
- Chest X-ray/CT: bilateral hilar lymphadenopathy, reticulonodular infiltrates
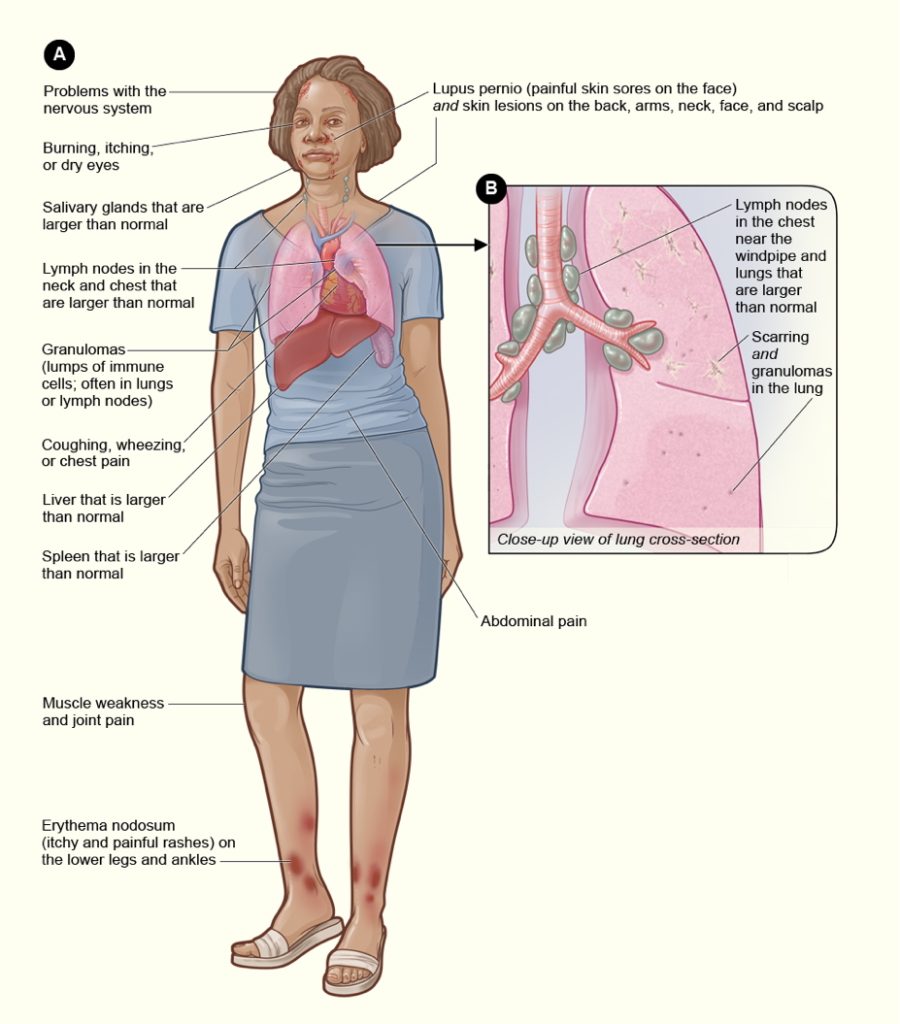
Clinical Features
- Pulmonary:
- Dyspnoea
- Dry cough
- Chest discomfort
- Restrictive lung pattern on spirometry
- Extrapulmonary:
- Lymphadenopathy (especially hilar)
- Skin: Erythema nodosum, lupus pernio
- Eyes: Uveitis, conjunctivitis
- CNS: Facial nerve palsy, seizures, meningitis
- Cardiac: Arrhythmias, cardiomyopathy
- Renal: Hypercalcaemia, nephrocalcinosis
Investigations
- Chest CT – Bilateral hilar lymphadenopathy ± interstitial lung disease
- Biopsy (e.g. via EBUS or transbronchial) – Confirms diagnosis by showing non-caseating granulomas
- Serum ACE – Often elevated
- Calcium – Hypercalcaemia or hypercalciuria in ~10%
- Pulmonary Function Tests – Restrictive pattern ± reduced DLCO
- Bloods – LFTs, U&E (check for hepatic/renal involvement)
Management
- First-line: Oral corticosteroids (e.g. prednisolone)
- Other options (if corticosteroids fail or not tolerated):
- Methotrexate
- Azathioprine
- Hydroxychloroquine
- Monitor lung function and extrapulmonary complications regularly
Prognosis
- 50–70% of patients experience spontaneous remission within 1–3 years
- 20–30% develop chronic or progressive disease (especially with pulmonary fibrosis)
- Increased long-term risk of:
- Pulmonary fibrosis and respiratory failure
- Lung cancer
- Ocular and CNS complications
Summary – Sarcoidosis
Sarcoidosis is a granulomatous disease affecting multiple organs, most commonly the lungs, and presents with non-caseating granulomas. Clinical features range from respiratory symptoms to systemic findings like lymphadenopathy and erythema nodosum. Diagnosis is made by imaging and confirmed by biopsy. While many cases resolve spontaneously, corticosteroids are the mainstay of treatment for symptomatic or progressive disease. For broader context, visit our Respiratory Overview page.