Table of Contents
Overview
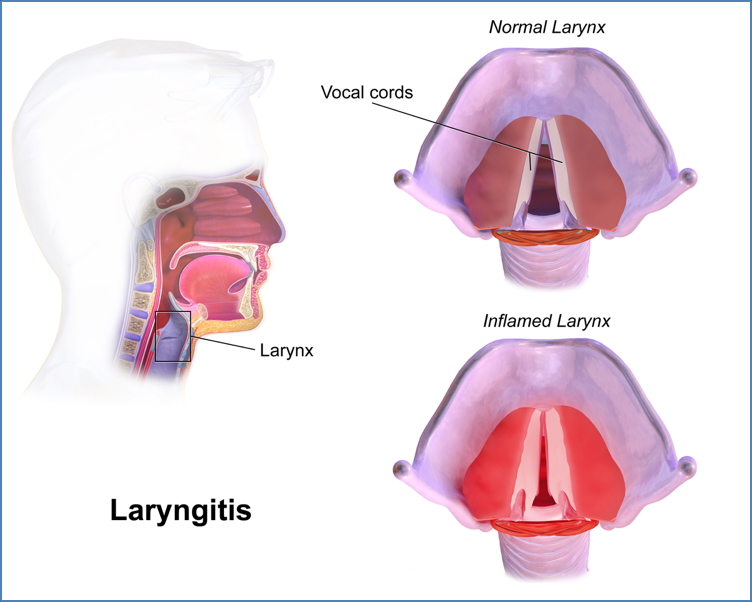
Laryngitis refers to inflammation of the larynx, most often resulting in hoarseness or loss of voice. It may present acutely as a self-limiting illness following an upper respiratory tract infection or develop chronically due to ongoing irritation or systemic conditions. Understanding the differences between acute and chronic forms—especially in terms of aetiology, presentation, and when to suspect more serious pathology—is critical for medical students and junior doctors.
Definition
Laryngitis is inflammation of the laryngeal mucosa, commonly affecting the vocal cords and resulting in voice changes. It is categorised as either acute or chronic depending on symptom duration.
Aetiology
Acute Laryngitis
- Viral (most common): Adenovirus, Influenza
- Bacterial: Group A Streptococcus (less common)
- Non-infective triggers:
- Acute vocal strain (e.g. yelling, singing)
- Toxic fume inhalation (e.g. smoke, chemical exposure)
Chronic Laryngitis
- Repeated episodes of acute laryngitis
- Long-term exposure to irritants: smoke, dust, chemical fumes
- Chronic voice misuse or occupational voice strain
- Chronic sinusitis with postnasal drip
- Gastro-oesophageal reflux disease (GORD)
- Chronic alcohol use
- Structural causes: hiatus hernia
Morphology / Pathophysiology
Acute
- Erythematous and oedematous true vocal cords
- Vascular injection
- Cord mobility typically remains normal
Chronic
- Thickened and erythematous cords
- Ulceration or granuloma formation
- May appear nodular
- Rule out laryngeal malignancy in persistent dysphonia

Clinical Features
Acute Laryngitis
- Often follows URTI
- Hoarseness (hallmark)
- Aphonia (loss of voice)
- Coughing attacks
- ± Dyspnoea if airway inflammation is significant
- Associated URTI symptoms (fever, sore throat, malaise)
Chronic Laryngitis
- Persistent dysphonia
- Globus sensation
- Frequent throat clearing
- Cough
- History of GORD, alcohol use, or smoking is common
Investigations
Usually clinical diagnosis based on history and physical exam
Consider further workup in:
- Chronic symptoms (>3 weeks)
- Unilateral symptoms
- High-risk features (smoking, alcohol use, weight loss)
Possible tests:
- Indirect laryngoscopy or flexible nasoendoscopy
- CT scan of neck (if mass suspected)
- Laryngopharyngeal pH monitoring (if GORD suspected)
Management
Acute Laryngitis
- Self-limiting: resolution in ~1 week
- Voice rest
- Hydration and humidification
- Avoid irritants (e.g. smoking, shouting)
- Antibiotics only if bacterial superinfection (e.g. concurrent streptococcal pharyngitis)
Chronic Laryngitis
- Eliminate irritants (e.g. smoking cessation, workplace adjustments)
- Treat contributing conditions (e.g. antisecretory therapy for GORD)
- Speech therapy (especially for vocal strain)
- ± Antibiotics or corticosteroids (if inflammation is significant)
Complications
- Vocal cord nodules or polyps
- Chronic dysphonia
- Airway compromise (rare in chronic cases)
- Laryngeal carcinoma (must be ruled out in persistent hoarseness)
Differential Diagnosis
- Vocal cord nodules or cysts
- Vocal cord paralysis
- Epiglottitis
- Laryngeal papillomatosis
- Reflux laryngitis
- Laryngeal carcinoma
Summary
Laryngitis refers to inflammation of the larynx, presenting acutely with hoarseness and URTI symptoms, or chronically with persistent dysphonia and throat discomfort. Acute laryngitis is typically viral and self-limiting, whereas chronic cases are often linked to irritants, GORD, or vocal overuse. Management focuses on addressing underlying causes, voice rest, and symptom relief. For broader context, visit our Respiratory Overview page.