Table of Contents
Overview – Psoriasis
Psoriasis is a chronic, immune-mediated skin condition characterised by well-demarcated, erythematous plaques with silvery scale. It is driven by T-cell–mediated inflammation and keratinocyte hyperproliferation, resulting in increased epidermal turnover and thickened plaques. Beyond the skin, psoriasis can present as a multi-system disorder with joint, nail, and gastrointestinal involvement. While not curable, effective treatments can provide substantial relief.
Aetiology
- Multifactorial: Genetic predisposition and immune dysregulation
- Environmental and lifestyle triggers:
- Emotional stress
- Skin trauma (Koebner phenomenon)
- Infections and some medications
Pathogenesis
- T-cell driven immune activation:
- Sensitised T lymphocytes infiltrate the skin
- Release of cytokines and growth factors → epidermal hyperplasia
- Stimulates:
- Keratinocyte proliferation (↑ turnover rate)
- Vascular proliferation
- Chronic inflammation
Morphology
Gross Appearance
- Classic plaques with:
- Silvery-white scales
- Well-demarcated margins
- Erythematous base
- Bilateral and symmetrical distribution
- Nail changes:
- Pitting
- Onycholysis (nail separation)
- Nail dystrophy
- Auspitz sign: pinpoint bleeding when scale is removed


2. CopperKettle, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
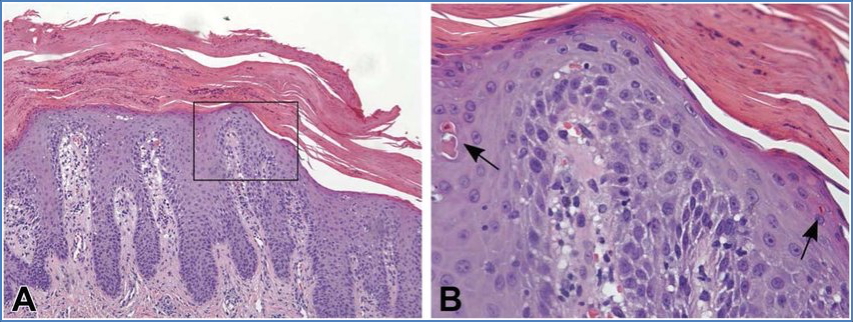
Histology
- Acanthosis (epidermal thickening with elongated rete ridges)
- Parakeratosis (retention of nuclei in stratum corneum)
- Neutrophilic microabscesses in the epidermis (Munro’s abscesses)
- Tortuous vessels in the papillary dermis
Clinical Features
- Can present at any age, including infancy
- Typically lifelong with relapsing-remitting course
- Lesions are:
- Not itchy (though pruritus may occur in some cases)
- Symmetrically distributed
- Common on:
- Elbows, knees, scalp, sacrum, nails
- Systemic manifestations:
- Psoriatic arthritis
- Myopathy
- Enteropathy
- Possible immunodeficiency features
Diagnosis
- Primarily clinical based on typical morphology and distribution
- Punch biopsy can confirm diagnosis if uncertain
Management
Topical
- Emollients
- Coal tar preparations
- Dithranol
- Salicylic acid
- Vitamin D analogues (e.g. calcipotriol)
- Topical corticosteroids
Phototherapy
- Sunlight may improve symptoms
- UVB phototherapy for widespread or refractory disease
Systemic (For Moderate to Severe Disease)
- Methotrexate
- Ciclosporin
- Acitretin
- Biologics may be used in severe or treatment-resistant cases
Prognosis
- Chronic, with no definitive cure
- Symptoms fluctuate in severity
- Management focuses on remission and symptom control
- Stress is a recognised exacerbating factor
Summary – Psoriasis
Psoriasis is a lifelong, immune-mediated condition presenting with well-demarcated, scaly plaques and often accompanied by systemic features such as nail changes and arthritis. It is diagnosed clinically and managed with topical therapy, phototherapy, and systemic agents depending on severity. For a broader context, see our Skin & Dermatology Overview page.